
![]()
Serratus Anterior Plane Block
The Superficial Serratus Anterior Plane Block (SAPB) is a technically simple and safe form of regional anaesthesia that can provide effective analgesia for up to 14 hours in patients with acute anterolateral rib fractures.
- Performed in the supine (or lateral decubitus) position, this block is particularly useful in the acute trauma patient
- Prospective studies have demonstrated reduced opioid consumption, improved pain scores, improved oxygen saturations, and reduce chronic pain with application of a single shot block
- Clinicians can use a superficial, deep, or mixed approach to application of local anaesthetic with respect to the serratus anterior plane. These authors advocate for a superficial approach due to its simplicity, reduced theoretical complication rate, and potentially longer duration of action
- In clinicians experienced with procedural ultrasound, the complication rate is low
Indications
- Two or more acute anterior, anterolateral, or lateral rib fractures
- Opioid analgesia and/or oxygen requirement
- Adjunctive analgesia in intercostal catheter (ICC) insertion
Contraindications
- Absolute:
- Local anaesthetic (LA) allergy
- Risk of LA toxicity (e.g. if other regional anaesthesia such as femoral nerve block already performed)
- Localised infection att site
- Relative:
- Inadequate assessment of sonoanatomy (e.g. obese patient)
Note that therapeutic anticoagulation is not a contraindication to SAPB administration.
Isolated posterior rib fractures may benefit more from other plane blocks such as the erector spinae (ESP) block.
Preparation
- Patients must be cardiac monitored in a resuscitation bay with IV access
- The patient is positioned supine, with their aim abducted to 90 degrees. Expose the entire chest wall
- We recommend a perpendicular-to-patient approach, as it allows comfort for the clinician and the best line of sight for ultrasound guidance. Position the machine in your line of vision on the opposite side of the block location
- Prepare the chest wall with 2% chlorhexidine solution
- Dilute 20ml of 0.75% ropivacaine (150mg) with 20ml normal saline for a total volume solution of 40ml (alternatively 40ml of 0.25% levobupivacaine, adhering to safe weight-based LA dosing)
- STOP before you block – confirm correct side of block
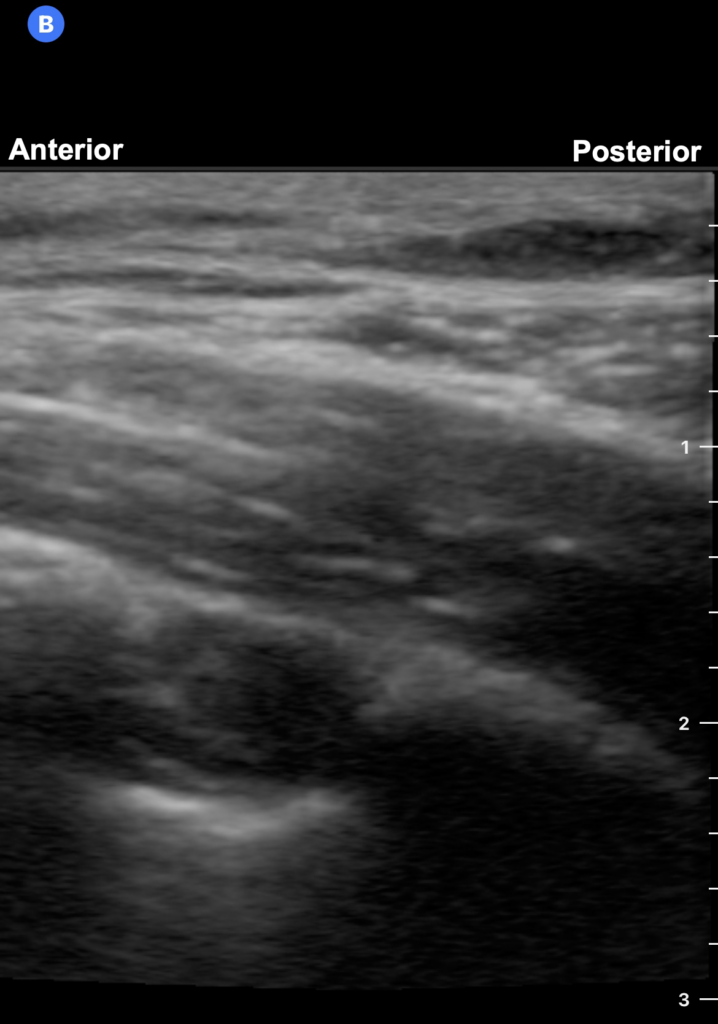
Sonoanatomy
- High frequency linear probe (ideally larger footprint) is placed in a transverse position in the mid-axillary line, at the level of the nipple
- Set your depth such that the pleural line and lung are in the bottom third of your image
- The latissimus dorsi is identifiable as a more superficial, triangular structure, extending over the serratus anterior muscle. If you are unable to visualise the latissimus dorsi, translate your probe more posteriorly (into the bed)
- The superficial plane lies in between the latissimus dorsi and serratus anterior muscles, and the deep plane extends between the serratus anterior and underlying ribs

Technique
- Use a perpendicular in-plane needle approach (anterior to posterior) and visualise needle tip at all times
- In the recommended superficial approach, the needle is advanced into the plane between the serratus anterior and latissimus dorsi
- With injection of LA, muscle layers should be seen to separate easily, with the fascial plane “peeling” open. Consider repositioning your needle if this is not seen, or if there is resistance to injection
Handy tips
- The thoracodorsal artery lies in the plane between the LD and SA muscles and should be identified using colour doppler before performing the block
- After creating a pocket of LA in the superficial serratus plane, re-position needle within pocket
References
- Blanco et al. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia [Internet]. 2013 Nov;68(11):1107–13
- Tekşen et al. Analgesic efficacy of the serratus anterior plane block in rib fractures pain: A randomized controlled trial. Am J Emerg Med [Internet]. 2021 Mar;41:16–20
- Miers J, Partyka C. Procedure: Serratus Anterior Block. LITFL
ULTRASOUND LIBRARY
POCUS, eFAST and basic principles

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

MBChB, FRCEM, PGCert (Public Health), PGDip (Medical Ultrasound), CCPU. UK Emergency & Intensive Care Registrar, ex-Melbourne. Fuelled by coffee and ultrasonic frequencies. @NishCherian