
![]()
Signe Brunnstrom

Anna Signe Sofia Brunnström (1898–1988) was a Swedish-American physical therapist, educator, and rehabilitation pioneer.
Brunnstrom’s clinical legacy includes clinical kinesiology, prosthetic rehabilitation, and stroke neurorehabilitation. She is remembered for the Brunnstrom approach and the recovery stages of hemiplegia her influence on the development of rehabilitation as an active, movement-based discipline.
Her early work focused on weight-bearing, lower-limb alignment, posture, and centre-of-gravity mechanics. This developed into a practical form of clinical kinesiology for physical and occupational therapists, linking anatomy and biomechanics directly to rehabilitation. During and after the Second World War, she applied the same movement-analysis principles to amputee and prosthetic rehabilitation, particularly pre-prosthetic training, standing balance, weight transfer, and gait.
In the 1950s and 1960s Brunnstrom extended this reasoning into adult hemiplegia. She observed that recovery after stroke often followed a recognisable sequence, from flaccidity through spasticity and mass synergy patterns toward more selective voluntary control. Her 1966 staging system gave therapists a practical framework for documenting change over time, while her treatment approach used reflexes, associated reactions, sensory stimulation, and synergies as early therapeutic entry points.
Biographical Timeline
- Born January 1, 1898 at Karlberg Castle, Solna, Stockholm, Sweden
- 1914 – Began studies for the Swedish studentexamen at age 16
- 1917 – Passed studentexamen and entered Gymnastiska centralinstitutet, Stockholm; training then conferred dual competence in physiotherapy and physical education.
- 1919 – Graduated from the Gymnastiska centralinstitutet with the title Gymnastikdirektor.
- 1920 – Moved to Bern, Switzerland, working with a Norwegian physiotherapist in private clinical practice.
- 1921 – Established her own Sjukgymnastik in Lucerne. Developed a reputation treating children with scoliosis and poliomyelitis, and ran remedial exercise programmes for working women.
- 1927 – Moved to New York City. Worked in exercise therapy at the Hospital for the Ruptured and Crippled, later the Hospital for Special Surgery.
- Late 1920s–1940s – Maintained private patients and worked intermittently for Metropolitan Life Insurance Company, teaching physical training and remedial exercise for women workers.
- 1931 – Entered Barnard College for chemistry and English. Studied part-time at New York University.
- 1934 – Became a United States citizen on November 26; officially changed her name from Anna Signe Sofia Brunnström to Signe Brunnstrom.
- 1935 – Earned Master of Arts at New York University.
- 1935 – Published “Faulty Weight Bearing“; an early marker of her clinical interest in posture, weight-bearing, and movement analysis.
- 1938–1942 – Appointed instructor of therapeutic exercise at New York University.
- 1941 – Applied through the American Red Cross for civilian military hospital service; assigned to the physical therapy department at Sheppard Field, Texas, with the Army Air Corps.
- 1943 – Enlisted in the US Navy; reported to the Navy Hospital at Mare Island, California, as officer in charge of physical therapy. Worked with Henry H. Kessler (1896–1978) and contributed to rehabilitation techniques for amputees and patients with peripheral nerve injury.
- 1944 – Promoted to lieutenant in the US Navy.
- 1945 – Awarded the US Navy Medal of Merit in recognition for wartime service.
- 1946 – Discharged from the Navy with the rank of lieutenant.
- 1948 – Joined the faculty of the Institute for Rehabilitation Medicine as a research associate on a Veterans Administration–NYU suction socket study.
- 1949 – Lead physical therapy role at the Kessler Institute of Rehabilitation, New Jersey
- 1951 – Awarded a Fulbright Lectureship to Greece; assisted in developing physical therapy training and amputee exercise programmes. Co-authored Leg Amputee: Pre-Prosthetic Training with Donald Kerr.
- 1955–1971 – Taught kinesiology to physical and occupational therapy students at the College of Physicians and Surgeons, Columbia University, New York.
- 1962 – Published Clinical kinesiology, the first American kinesiology text written specifically for physical and occupational therapy students.
- 1965 – Received the Marian Williams Research Award from the American Physical Therapy Association.
- 1970 – Published Movement therapy in hemiplegia: a neurophysiological approach, her landmark text on sequential motor recovery after stroke.
- 1973 – Received the University Citation of the State University of New York at Buffalo
- 1974 – Appointed honorary member of the Union of Swedish Physical Therapists.
- 1987 – APTA renamed its Award for Excellence in Clinical Teaching in her honour as the Signe Brunnstrom Award for Excellence in Clinical Teaching.
- Died on February 21, 1988 at Darien, Connecticut, USA
Key Medical Contributions
Clinical kinesiology and movement analysis
Brunnstrom’s work in hemiplegic movement therapy developed from a long-standing interest in clinical movement analysis. Before she became associated with stroke rehabilitation, she was already writing about posture, weight-bearing, lower-limb alignment, and the relationship between segmental mechanics and functional movement.
In her 1935 paper on faulty weight-bearing, she treated weak arches and faulty foot posture not as isolated foot problems, but as disturbances involving the feet, legs, pelvis, spine, shoulders, and head. She emphasised individual assessment of malalignment rather than a prescription of corrective exercises.
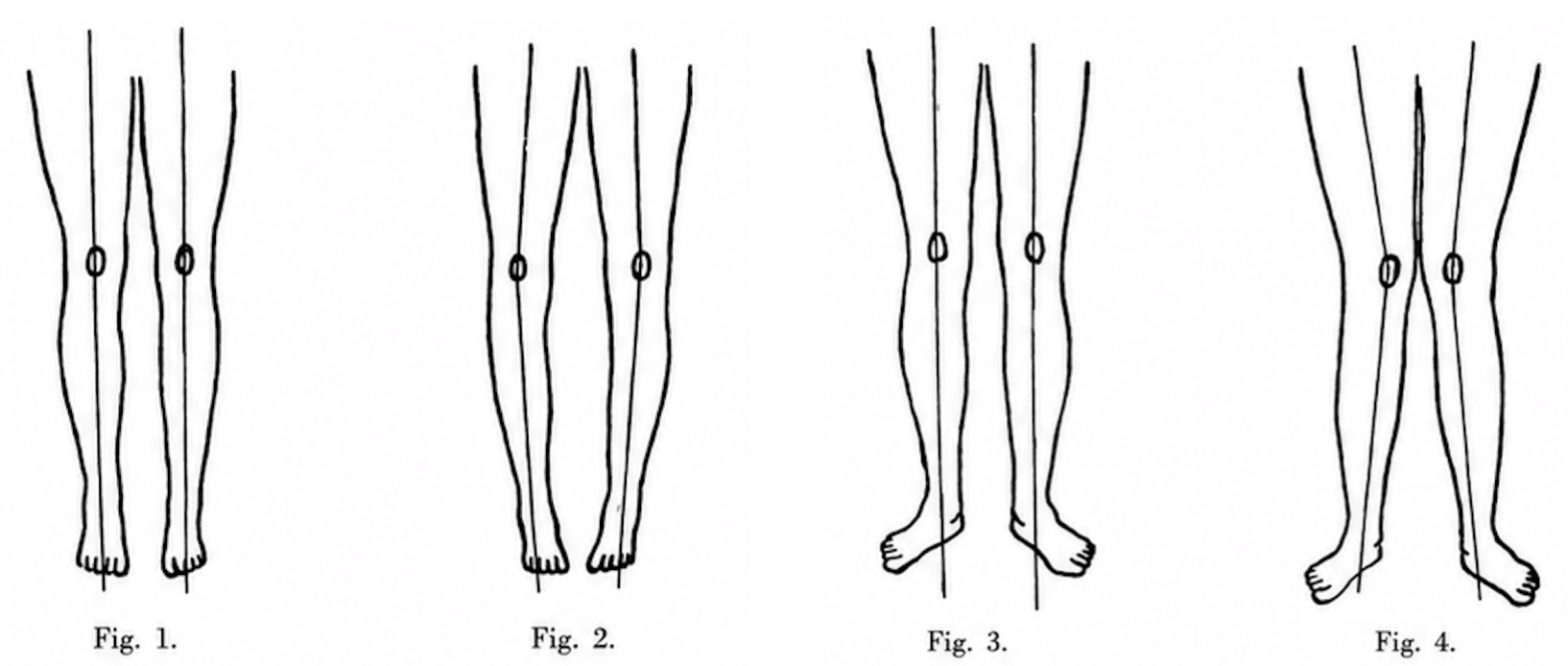
Fig. 1. Correct weight bearing. Weight is transmitted through thigh and leg in a straight line to the foot and evenly distributed to the sole of the foot.
Fig. 2. Thighs outward rotated, weight too much on outer border of feet. The gait is clumsy and the individual swaddles from side to side.
Fig. 3. Feet everted, thighs straight. Weight falls too much on inner side of feet, tending to flatten the arch.
Fig. 4. Feet everted, thighs inward rotated. Weight is borne too much on the inner border of the feet flattening the arch. Brunnstrom 1935
In 1954 she published centre-of-gravity line in relation to the ankle joint reviewing standing, balance, posture training, and artificial limb use. Brunnstrom challenged the conventional “plumbline” model of ideal standing posture proposing that in natural standing, the body’s centre of gravity falls anterior to the ankle joint. Brunnstrom linked biomechanical analysis to clinical practice, especially posture training and prosthetic rehabilitation.
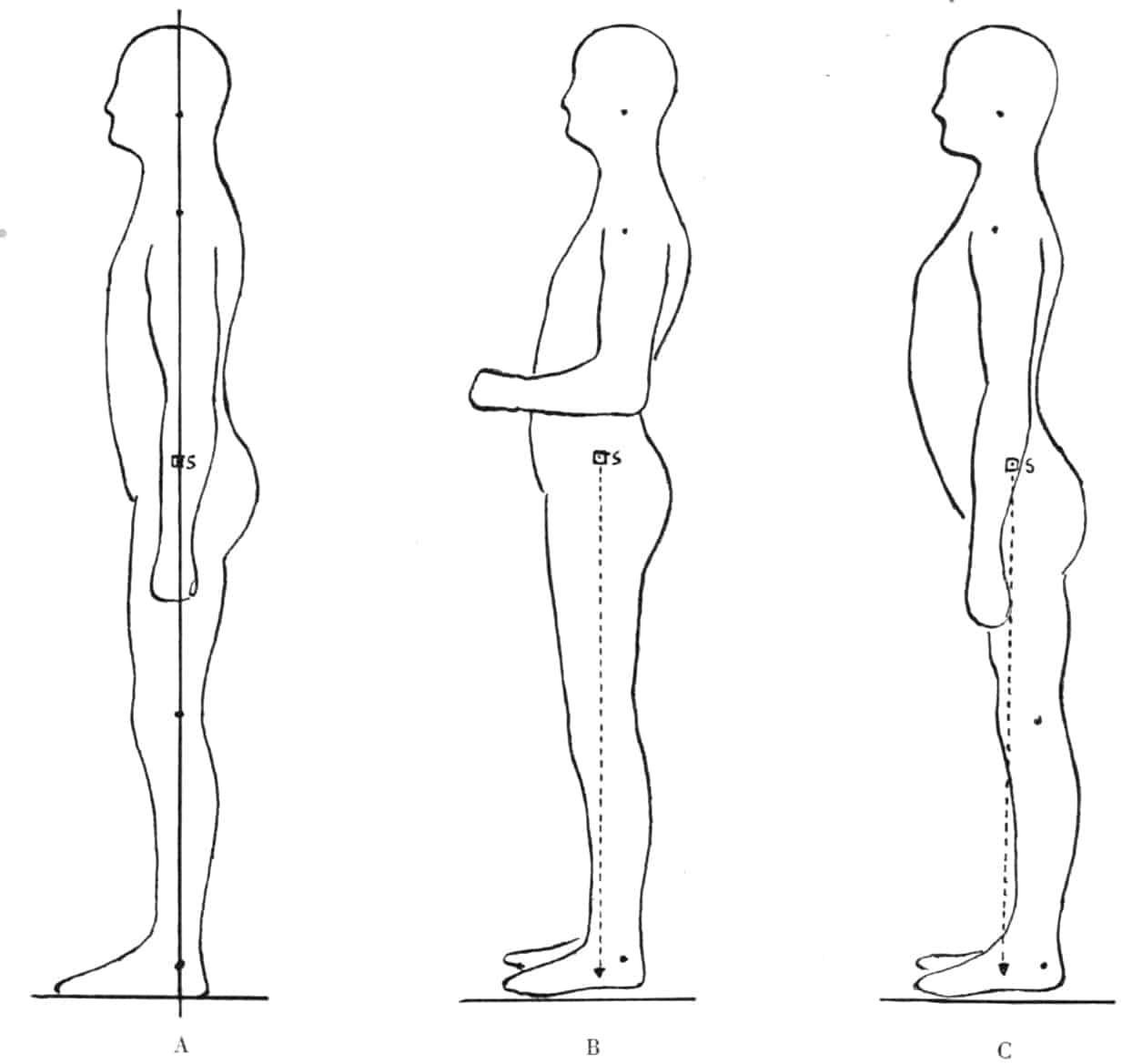
A. Perpendicular standing, adopted as a basic position and was (misleadingly) called Normalstellung.
B. Comfortable Posture (Bequeme Haltung)
C. Military position (Militärische Stellung) Brunnstrom 1954
Amputee and prosthetic rehabilitation
During and after the Second World War, Brunnstrom applied therapeutic exercise, posture analysis, gait mechanics, and balance training to the rehabilitation of patients with limb loss. During her wartime service in the United States Navy placed she combined physical therapy with surgical aftercare, prosthetic fitting, gait retraining, and restoration of function.
After the war she continued prosthetic research and teaching, including work at the Kessler Institute, the Veterans Administration, and during her Fulbright Lectureship in Greece. Her 1951 article “Amputee Training in Greece” gives a vivid account of the practical problems encountered. Many amputees had artificial limbs but no effective training in balance, weight transfer, or gait. At the Psychico Amputee Hostel near Athens, she developed group-based pre-prosthetic and prosthetic exercises, including trunk flexibility, lateral weight shift, balance over the prosthesis, stair practice, and outdoor functional training.
Prosthetic walking was not treated as a technical problem of limb fitting alone, but as a whole-body problem involving posture, symmetry, balance, confidence, repetition, and functional use. Her publications with Donald Kerr, including Leg Amputee: Pre-Prosthetic Training and Training of the Lower Extremity Amputee exemplified this approach.
Associated reactions and early neurorehabilitation
In 1956, Brunnstrom published “Associated reactions of the upper extremity in adult patients with hemiplegia; an approach to training”. She noted that in adult hemiplegia, associated reactions were involuntary movements or increased tone in the affected limb during effort elsewhere in the body. Brunnstrom interpreted these reactions as clinical signs of persisting motor organisation. They revealed movement patterns that could be elicited when isolated voluntary movement was absent or severely limited.
Brunnstrom argued that associated reactions, reflexes, sensory stimulation, resistance, and mass movement patterns were useful as transitional tools. They could help the patient experience movement, generate muscle activity, and begin the progression from reflexive or semi-voluntary mass patterns toward more selective voluntary control.
Sequential motor recovery after stroke
Brunnstrom’s best-known clinical contribution was her description of sequential motor recovery in adult hemiplegia. In her 1966 paper Motor testing procedures in hemiplegia: based on sequential recovery stages she argued that motor recovery commonly began with flaccidity, progressed through stages marked by spasticity and stereotyped patterns, and, in more favourable cases, advanced toward diminishing spasticity and increasingly selective voluntary control.
Brunnstrom did not simply describe abnormal movement but provided therapists a way to observe, classify, and document recovery. She emphasised that progress varied between patients, that recovery could arrest at any stage, and that the upper and lower limbs could recover unevenly. Her testing format separated the upper limb, hand, trunk, lower limb, standing, walking, and gait, making the stages both a clinical record and a guide to treatment planning.
The resulting Brunnstrom recovery stages provided clinicians with a vocabulary for describing post-stroke motor change. This included flaccidity, emerging spasticity, synergy-dominated movement, movement outside synergy, and eventual near-normal coordination. This framework became one of the most recognisable clinical assessment systems in stroke rehabilitation.
The Brunnstrom approach to movement therapy
Brunnstrom’s staged description of hemiplegic recovery became the basis for the broader Brunnstrom approach, or Brunnstrom movement therapy. The approach linked assessment and treatment. The patient’s recovery stage indicated both the movement available and the next therapeutic challenge.
One defining feature was Brunnstrom’s therapeutic use of limb synergies. In early stages, patients might only be able to move within stereotyped flexor or extensor patterns. Brunnstrom accepted these patterns as part of the recovery sequence and, in selected circumstances, used them to elicit movement. Later treatment aimed to help the patient move out of synergy, combine joint actions more selectively, and progress toward functional voluntary control.
Controversy, and modern interpretation
Brunnstrom stages remain recognisable in stroke rehabilitation and research as measures of motor recovery, including studies of spasticity, neurophysiology, functional independence, and imaging-based prognosis.
Her treatment principles also became part of the historical Brunnstrom–Bobath/NDT controversy. In simple terms, Brunnstrom accepted abnormal synergies and associated reactions as possible early routes into movement, while Bobath emphasised inhibition of abnormal tone and facilitation of more normal movement patterns. The disagreement reflected not only different techniques, but different assumptions about recovery, spasticity, and therapeutic progression.
Today, the Brunnstrom approach is best understood as an important historical and clinical framework. Contemporary stroke rehabilitation generally favours well-described, evidence-based components such as intensity, repetition, task-specific practice, strengthening, gait training, and individualised goals. Brunnstrom remains important for providing therapists with a structured way to observe, document, and work with the evolving motor behaviour of patients after stroke.
Major Publications
- Brunnstrom S. Faulty Weight Bearing: With Special Reference to Position of Thigh and Foot. The Physiotherapy Review 1935; 15(3): 83-87
- Brunnstrom S. Comparative strength of muscles with similar function; a study on peripheral nerve injuries of the upper extremity. Physiotherap Rev. 1946 Mar-Apr;26:59-65.
- Brunnstrom S. Walking training of the amputee; some biomechanical considerations. Physiotherap Rev. 1947 May-Jun;27(3):147-55
- Brunnstrom S, Kerr D. Leg amputee: pre-prosthetic training. 1951
- Brunnstrom S. Amputee training in Greece. Phys Ther Rev. 1951 Oct;31(10):419-26.
- Brunnstrom S. Center of gravity line in relation to ankle joint in erect standing, application to posture training and to artificial legs. Phys Ther Rev. 1954 Mar;34(3):109-15.
- Kerr D, Brunnstrom S. Training of the Lower Extremity Amputee. 1956
- Brunnstrom S. Associated reactions of the upper extremity in adult patients with hemiplegia; an approach to training. Phys Ther Rev. 1956 Apr;36(4):225-36.
- Brunnstrom S. Recording gait patterns of adult hemiplegic patients. Phys Ther. 1964 Jan;44:11-8.
- Brunnstrom S. Clinical kinesiology. 1962 [2e 1966, 3e 1972, 4e 1984, 6e 2011]
- Brunnstrom S. Walking preparation for adult patients with hemiplegia. Phys Ther. 1965 Jan;45:17-29.
- Brunnstrom S. Motor testing procedures in hemiplegia: based on sequential recovery stages. Phys Ther. 1966 Apr;46(4):357-75.
- Brunnstrom S. Movement therapy in hemiplegia: a neurophysiological approach. 1970 [2e 1992]
References
Biography
- Schleichkorn J. Signe Brunnstrom: Physical Therapy Pioneer, Master Clinician and Humanitarian. 1990
- Biographical Sketch of Signe Brunnstrom, 1898–1988. In: Houglum PA, Bertoti DB. eds. Brunnstrom’s Clinical Kinesiology, 6e. F. A. Davis Company; 2012
- Anna Signe Sofia Brunnström. Svenskt kvinnobiografiskt lexikon
Eponymous terms
- Naghdi S, Ansari NN, Mansouri K, Hasson S. A neurophysiological and clinical study of Brunnstrom recovery stages in the upper limb following stroke. Brain Inj. 2010;24(11):1372-8.
- Pollock A, Baer G, Campbell P, Choo PL, Forster A, Morris J, Pomeroy VM, Langhorne P. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst Rev. 2014 Apr 22;2014(4):CD001920.
- Huang CY, Lin GH, Huang YJ, Song CY, Lee YC, How MJ, Chen YM, Hsueh IP, Chen MH, Hsieh CL. Improving the utility of the Brunnstrom recovery stages in patients with stroke: Validation and quantification. Medicine (Baltimore). 2016 Aug;95(31):e4508.
- Ottosson A. Signe Brunnström’s Influence on US Physical Therapy, Physical Therapy, 2021; 101(8): 156
- Yang SN, Kim DY. Comparing the Effectiveness of Physical Rehabilitation Interventions for Post-Stroke Function and Mobility Recovery: A Meta-Analysis. Brain Neurorehabil. 2023 Jul 13;16(2):e17.
- Uchiyama Y, Domen K, Koyama T. Brain regions associated with Brunnstrom and functional independence measure scores in patients after a stroke: a tract-based spatial statistics study. J Phys Ther Sci. 2023 Mar;35(3):211-216.
- Borzelli D, De Marchis C, Quercia A, De Pasquale P, Casile A, Quartarone A, Calabrò RS, d’Avella A. Muscle Synergy Analysis as a Tool for Assessing the Effectiveness of Gait Rehabilitation Therapies: A Methodological Review and Perspective. Bioengineering (Basel). 2024 Aug 5;11(8):793.
Eponym
the person behind the name

Studying for Bachelor of Science (Occupational Therapy) at Curtin University
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
