
![]()
Sternoclavicular Joint Dislocation
Sternoclavicular joint dislocation is a relatively uncommon injury that can be easily missed or misdiagnosed. Bilateral posterior sternoclavicular joint dislocation is particularly uncommon.
The importance in determining the direction of dislocation is emphasised by the dichotomy of management. Hence, a thorough history and examination, especially looking for evidence of compression of retrosternal structures, is paramount. Specialised sternoclavicular X-ray views should be supplemented by CT/MRI if clinical suspicion is high. Posterior dislocations necessitate prompt orthopedic referral.
Case Report
A 30 year old man presented to ED with bilateral “shoulder pain” after a quad bike accident. The patient took a corner at high-speed landing heavily on his right shoulder and crushed by the bike landing on his left shoulder.
- On presentation, ABCs were intact GCS 15 he ambulated into the department. He had no dysphonia, dysphagia or dyspnoea.
- On examination – both right and left shoulders were dislocated anteriorly.
- On arrival into the department and XR was performed and both shoulders relocated.
- Subsequent examination revealed swelling and tenderness over both sternoclavicular joints and the patient was unable to abduct either shoulder actively despite glenohumeral enlocation. Passive movement of the shoulders was limited by pain “over the collarbone”, although the clavicles themselves were only tender near their junction with the sternum. Specifically, the AC joints and humerus were non-tender and arm neurovascular status was normal.

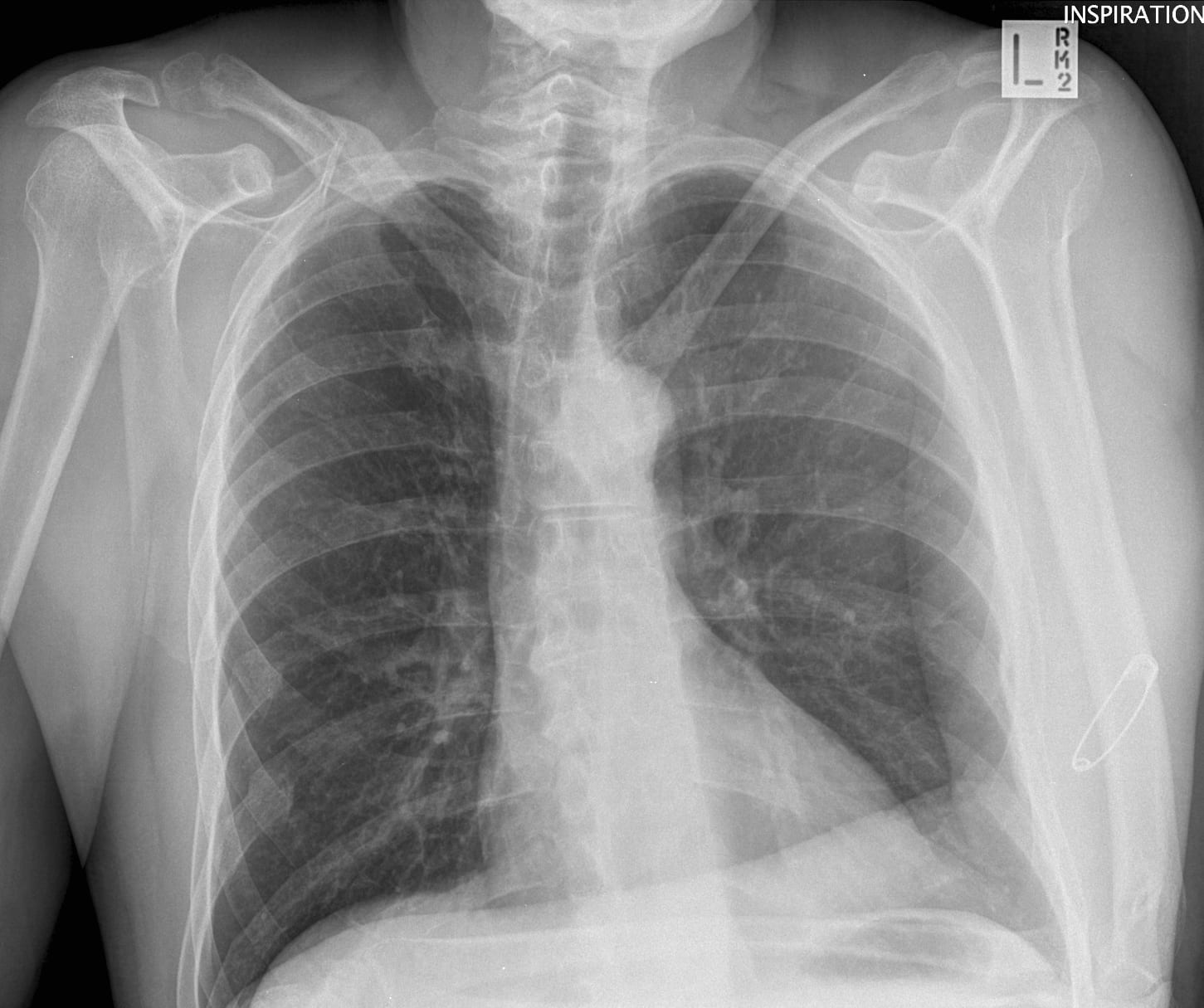
The Chest XR was reported as ‘normal’…
However in light of the high clinical suspicion for sternoclavicular joint injury; continued anterior chest pain and failure in shoulder abduction special plain film tomography views of both SC joints was performed:

There is widening of the right sternoclavicular joint when compared to the left side. This appearance is suspicious for subluxation/dislocation. There is probable subtle widening of the left sternoclavicular joint as well. Several well-corticated bone ossicles are noted in the vicinity of the sternoclavicular joints bilaterally.
CT scan confirmed superior dislocation of bilateral sternoclavicular joints with associated fracture of the left 1st rib anteriorly
Anatomy of the sternoclavicular joint
- The sternoclavicular joint is a diarthodial saddle-type joint which provides a pivot for the shoulder girdle on the trunk.
- The joint capsule is reinforced anterioposteriorly by the anterior and posterior sternoclavicular ligaments. Superomedially the joint is reinforced by the interclavicular ligament which joins both the upper border of both clavicles to the suprasternal notch.
- The clavicle is also bound to the first costal cartilage and the first rib by the costoclavicular ligament.

Clinical Presentation
Incidence
- Sternoclavicular dislocations account for 3% of all shoulder girdle injuries.
- 95% of SCJ dislocations are unilateral and anterior dislocations are far more common than posterior dislocations due to the weaker anterior sternoclavicular ligament (ratio 9:1). Bilateral superior dislocations, as in the case above, are rarely described.
Mechanism of Injury
- Dislocations of the SCJ generally occur following a fall on the outstretched hand or a direct blow to the shoulder. Sporting injuries and motor vehicle accidents account for the most causes of SCJ dysfunction. However, they can also occur without any history of injury.
- Patients commonly present with pain and swelling in the proximal sternum and sternoclavicular region. The pain will be exacerbated by lateral shoulder compression, arm movements, deep breathing or coughing.
- Patients often laterally flex their neck towards the affected side to relieving pressure on the SCJ. Asymmetry is best appreciated when viewed from above the patient’s head.
- Additional symptoms include dysphonia, dysphagia or dyspnoea.
Diagnostic Imaging
- Plain X-ray: standard views may not provide a definitive diagnosis. Alternate views such as ‘serendipity view‘ (40-degree cephalic tilt) may provide more information.
- CTA or MRA to determine direction of dislocation and potential for vascular compromise. A contrast study is required for definitive evaluation of surrounding structures.
Complications
Many complications have been reported in the literature related to retrosternal (posterior) dislocation of the medial end of the clavicle including:
- Subclavian compression and laceration
- Mediastinal compression
- Pneumothorax
- Oesophageal rupture
- Myocardial conduction abnormalities
- Brachial plexopathy
- Tracheal tear
- Thoracic outlet syndrome
Management
Simple sprain of the SCJ
- Patients will complain of mild to moderate pain and there will be no joint instability on clinical examination.
- Conservative treatment with ice, analgesia, shoulder sling for immobility will lead to complete recovery in 1 week.
- Subluxation of the SCJ will require the application of a clavicular splint or sling for 3 to 6 weeks
Anterior SCJ Dislocations
- Anterior sternoclavicular dislocations are usually managed nonoperatively.
- The clavicle often stabilises in its subluxed position, with asymmetrical ventral protrusion of the affected side. The arm should be rested in a sling which will assist in the reduction of pain. Patients generally experience a good pain-free functional outcome at 2-3 weeks. Very rare complications include chronic pain, periarticular calcifications with ankylosis and progressive deformity.
- Closed reduction may be indicated in rare circumstances where the patient is engaged in strenuous upper limb activities causing a painful SCJ. It is however, often unsuccessful. The application of direct pressure over the medial end of the clavicle may also reduce the joint.
Posterior SCJ Dislocations
- Posterior sternoclavicular dislocations should always be reduced in theatre because of the associated risk to intrathoracic and superior mediastinal structures.
Methods of reduction
The initial treatment of choice is a closed reduction. Various methods have been described:
- Classical: Patient positioned supine with a towel/sandbag between scapulae. Sedation is administered and traction is applied to the abducted arm with simultaneous extension. This has an 80% success rate.
- Buckerfield and Castle: While shoulders are pushed posteriorly by an assistant, the ipsilateral arm is adducted against the torso and caudal traction is applied.
- Towel Clip: Anterior traction force can be applied to clavicle by percutaneously applied towel clip, often used with one of the above methods.
- A figure of eight sling is applied after the reduction for 4-6 weeks to allow for ligamentous healing.
If the SCJ becomes chronically unstable or if closed reduction is unsuccessful, then open reduction is indicated.
Discussion
Traumatic sternoclavicular joint dislocation is an uncommon condition whose diagnosis is often missed. The importance in determining the direction of dislocation is emphasised by the dichotomy of management. The posterior version of this dislocation has been associated with multiple complications and owing to the rarity of this injury, there is a relative lack of familiarity with the diagnosis, surgical anatomy and treatment options. [Reference]
A thorough history and examination, especially looking for evidence of compression of retrosternal structures, is paramount. Specialised sternoclavicular X-ray views should be supplemented by CT/MRI if clinical suspicion is high. Posterior dislocations necessitate prompt orthopedic referral.
Example of a Unilateral Posterior Sternoclavicular Dislocation

Further reading
LITFL
- Davidson J et al. CT Case 035. LITFL
FOAM
Publications
- Gazak S, Davidson SJ. Posterior sternoclavicular dislocations: two case reports. J Trauma. 1984 Jan;24(1):80-2
- Wirth MA, Rockwood CA Jr. Acute and Chronic Traumatic Injuries of the Sternoclavicular Joint. J Am Acad Orthop Surg. 1996 Oct;4(5):268-278
- Jougon JB, Lepront DJ, Dromer CE. Posterior dislocation of the sternoclavicular joint leading to mediastinal compression. Ann Thorac Surg. 1996 Feb;61(2):711-3.
- Brinker MR, Bartz RL, Reardon PR, Reardon MJ. A method for open reduction and internal fixation of the unstable posterior sternoclavicular joint dislocation. J Orthop Trauma. 1997 Jul;11(5):378-81.
- O’Connor PA, Nölke L, O’Donnell A, Lingham KM. Retrosternal dislocation of the clavicle associated with a traumatic pneumothorax. Interact Cardiovasc Thorac Surg. 2003 Mar;2(1):9-11.
- Mirza AH, Alam K, Ali A. Posterior sternoclavicular dislocation in a rugby player as a cause of silent vascular compromise: a case report. Br J Sports Med. 2005 May;39(5):e28.
- Hoekzema N, Torchia M, Adkins M, Cassivi SD. Posterior sternoclavicular joint dislocation. Can J Surg. 2008 Feb;51(1):E19-20
- Groh GI, Wirth MA. Management of traumatic sternoclavicular joint injuries. J Am Acad Orthop Surg. 2011 Jan;19(1):1-7.
- Sewell MD, Al-Hadithy N, Le Leu A, Lambert SM. Instability of the sternoclavicular joint: current concepts in classification, treatment and outcomes. Bone Joint J. 2013 Jun;95-B(6):721-31.
- Balcik BJ, Monseau AJ, Krantz W. Evaluation and treatment of sternoclavicular, clavicular, and acromioclavicular injuries. Prim Care. 2013 Dec;40(4):911-23
- Deren ME, Behrens SB, Vopat BG, Blaine TA. Posterior sternoclavicular dislocations: a brief review and technique for closed management of a rare but serious injury. Orthop Rev (Pavia). 2014 Mar 12;6(1):5245.
- Saltzman MD, Mercer DM, Bertelsen A, Warme WJ, Matsen FA 3rd. Bilateral Posterior Sternoclavicular Dislocations. Radiol Case Rep. 2016 Oct 4;4(1):256
[cite]
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |