
![]()
Thomas test
Description
The Thomas test is a physical examination test, first described in 1875 by the Welsh bonesetter Hugh Owen Thomas (1834–1891). The test was used to diagnose hip flexion contracture and determine the duration of the disease process.
The modified Thomas test is most often used to asses and evaluate flexibility of the hip flexors including the iliopsoas muscle group, quadriceps, pectineus, gracillus, tensor fascia latae and sartorius.
Patient lies supine on the examination table and holds both knees to the chest ensuring the lumbar spine is flexed and flat on the table. The patient then lowers the tested limb (extends hip) towards the table, whilst holding the contralateral hip and knee in maximal flexion to stabilize the pelvis and flatten out the lumbar lordosis. Measurements are taken:
- Length of the iliopsoas (angle of the hip flexion)
- Passive length of the quadriceps (knee flexion angle)
- Tensor fascia latae/Iliotibial band flexibility (hip abduction angle relative to the femur and angle of the pelvis)
History – the Original Thomas Test
1875 – Hugh Owen Thomas published ‘Diagnosis of inflammation of the hip joint‘.
I have tested it during ten years, and never once has it failed in enabling me to detect the disease at even so early a stage as the first week or day, if there is any effusion into the joint…it is is of value to the surgeon in the cases of children in particular…as this method demonstrates two invariable symptoms of hip joint inflammation, flexion of the hip joint, and curve of the spine. Plate 3 illustrates the manipulation in this diagnostic method.
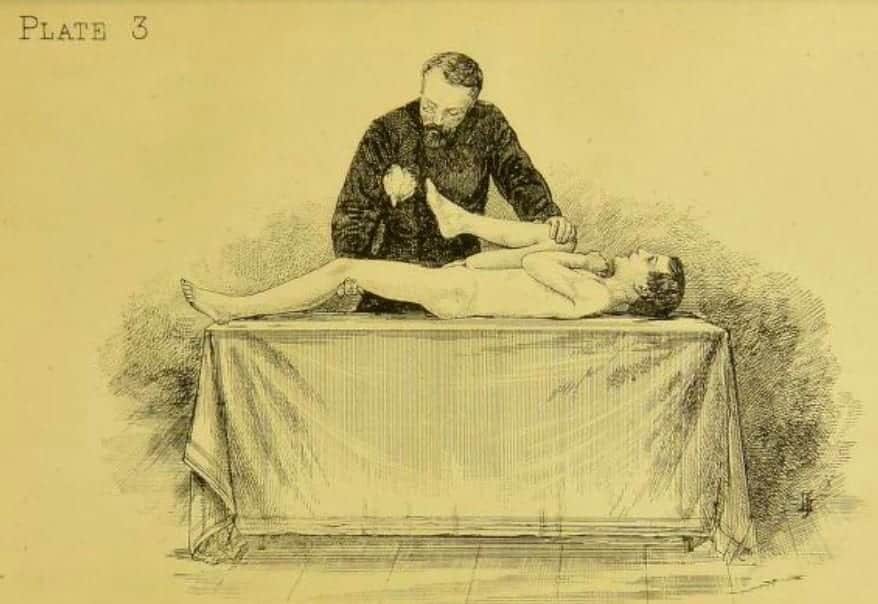
Having undressed the patient and laid him on his back upon a table or other hard plane surface, the surgeon takes the sound limb and flexes it, so that the knee joint is in contact with the chest. Thus he makes certain that the spine and back of the pelvis are lying flat on the table; an assistant maintains the sound limb in this fixed position; the patient is then urged to extend, as far as he is able, the diseased limb, and this he will be able to do in a degree varying with the previous duration of the affection. While the patient is retained in this position the operator will be able readily to note a rigid cord corresponding to the origin of the adductors, which are invariably the first to shorten.
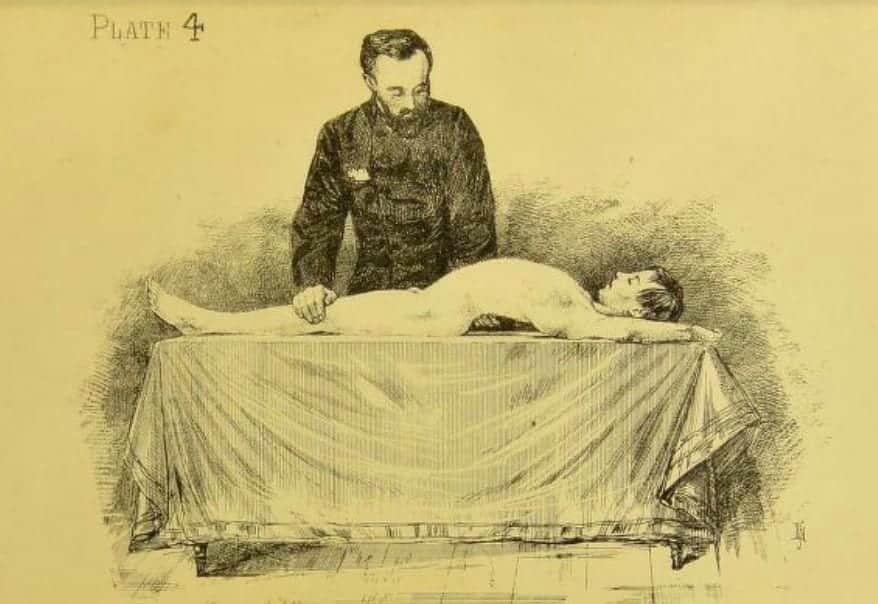
On releasing the sound limb from its flexed position on the chest, the patient may be able to apparently extend the limb, but a compensatory curve of the spine is formed. Plate 4 represents the patient’s spine as curved when the leverage of the sound limb is taken off the pelvis. The flexion here shown indicates a period of many months. This diagnostic manipulation enables the surgeon to note at a glance the amount of flexion and, with practice, soon be able to guess the previous duration of the disease.

Plate 6 shows the same case with the leverage of the sound limb fixing the pelvis, and so controlling the spine. In cases of abscess connected with the pelvis or spine, this curving of the spine is absent when the patient makes an attempt to extend the limb, though the hip may be flexed to a greater or less degree. Here we have contraction of the flexors without hip disease.

Plate 23 published in 1876, demonstrates an improvement to the diagnostic method. The forearm of the sound side is used as a means of fixing the sound lower limb on to the trunk during examination of diseased side.
Associated Persons
- Hugh Owen Thomas (1834 – 1891)
Alternative names
- Iliacus Test
- Iliopsoas Test
References
- Thomas HO. Diseases of the hip, knee, and ankle, joints, with their deformities: treated by a new and efficient method. 1876: 16-26
- Harvey D. Assessment of the flexibility of elite athletes using the modified Thomas test. Br J Sports Med 1998 32: 68-70.

eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |