
![]()
Winter is Coming
aka ECG Exigency 016
A 54-year old man presents by private vehicle to the Emergency Department with chest discomfort he described as “heartburn.” The pain is substernal and non-radiating. He is also mildly diaphoretic.
There is no history of diabetes, hypertension, high cholesterol, or coronary artery disease. On arrival he is resting comfortably, with the following vitals: heart rate 56, blood pressure 125/82, respirations 18 per minute and unlaboured, oxygen saturation 100% on room air. His ECG is shown below:
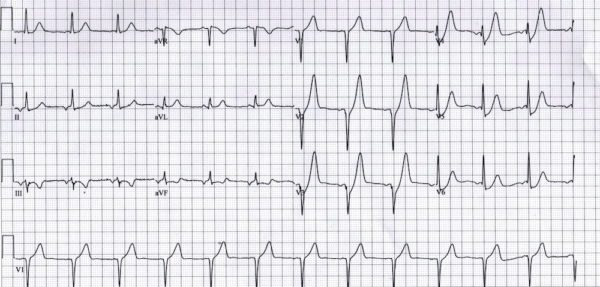
Q1. Describe the ECG.
Answer and Interpretation
- Ectopic atrial rhythm: inverted P waves in II, III, aVF
- Rate 75 bpm
- Normal axis: +30 degrees, QRS complexes upright in leads I + II
- Normal intervals
- 1mm ST-segment elevation in aVR
- Upsloping ST-segment depression in V2-V6
- Tall, prominent, symmetric T waves throughout the precordial leads
Q2. What is the significance of these ECG findings?
Answer and Interpretation
These ST and T waves abnormalities are known as de Winter T-waves

This ECG finding:
- Is specific for left anterior descending artery (LAD) occlusion.
- Represents ~2% of LAD occlusions.
- May persist until the culprit artery is opened (making it a STEMI equivalent) or may evolve into an anterior STEMI.
Q3. How would you manage this patient?
Answer and Interpretation
This patient needs to be managed as a STEMI with analgesia, nitrates, oxygen, aspirin, heparin and (most importantly) emergent PCI or thrombolysis!
Q4. Can you guess what happened next?
Answer and Interpretation
The patient was admitted for emergent PCI.
- Angiography revealed a 100% mid-LAD occlusion, which was successfully stented.
- His troponin peaked at 197 ng/mL.
- The patient was eventually discharged with a normal ejection fraction.
Take Home Points
- The de Winter ECG pattern is a recently-described STEMI equivalent that emergency physicians and paramedics must be aware of.
- These patients typically have critical stenosis of the LAD requiring emergent PCI or thrombolysis.
- Lack of familiarity with these ECG findings may lead to reluctance to activate the cath lab and unacceptable delays in reperfusion.
- Remember that in many cases the de Winter pattern persisted until after the target artery was opened. Don’t wait for serial ECGs to evolve into a more easily recognisable STEMI pattern (which may never happen): activate the cath lab now!
References
- Hampton, JR. The ECG In Practice, 6e
- Mattu A, Brady W. ECG’s for the Emergency Physician 1
- Mattu A, Brady W. ECGs for the Emergency Physician 2
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric, 6e
- Wagner, GS. Marriott’s Practical Electrocardiography 12e
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF

CLINICAL CASES
ECG EXIGENCY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
excellent, Ed.
may i suggest a few more points?
1. reciprocal changes inferiorly, with ST set depression, and flipped T’s
2. hyper acute T’s in V1-4 (you mentioned) alone would be worrisome for acute OMI (occlusive MI).
3. mattu has said the an upright T in V1, esp if its higher than the T in V6 (unless its all old), is worrisome.
4. very poor R-wave progression V1-3.
thank you for this excellent example of de Winters.
tom