
![]()
Zany Zipper
aka Pediatric Perplexity 011
A 6-year old boy presents to ED in agony after entrapping his penis in the zipper of his new jeans. He is very distressed, unable to lay still or co-operate, and every movement of his legs makes him scream in pain as the fabric tugs on his sequestered foreskin. At this stage, you cannot get close enough to see where exactly within the zipper mechanism he is entrapped.
Questions
Q1. What would be your initial approach to the management of this patient?
Answer and interpretation
There are four main aspects of management to consider:
- analgesia and sedation
- gaining access to the operation site
- local anaesthesia
- extrication from the zipper
Analgesia and Sedation
- This patient will need adequate analgesia and/or sedation if he is to be successfully examined and treated
- We used intranasal fentanyl 1.5 mcg/kg plus inhaled nitrous oxide
- Procedural sedation (e.g. ketamine) or general anaesthesia may be required
Gain Access to the Operation Site
- Cut off the trousers with trauma scissors, leaving only the zipper in place around the penis
- This will enable better visualisation of the entrapment and minimize further trauma due to the weight of the trousers pulling on the foreskin
Local Anaesthetic
- Local anaesthetic (e.g. lidocaine without adrenaline) may be infiltrated directly into the entrapped skin to facilitate removal
- Topical local anaesthetic (e.g. EMLA) may provide effective anaesthesia when applied liberally to the entrapped skin. The disadvantage of this technique is that it takes 45-60 minutes to take effect (which is a long time to sit with your penis caught in a zipper!)
- Dorsal penile block is another alternative, probably best reserved for difficult entrapments involving large amounts of skin
- As with any paediatric procedure, the benefits of infiltrating with local anaesthetic must be weighed against the pain of the injection itself
Extrication from the zipper… see Q2!
Q2. What techniques can be employed to extricate him from the zipper?
Answer and interpretation
The method of removal depends on where the genital skin is entrapped. The skin of the foreskin or scrotum may become stuck in two main sites:
- Between the teeth of the zipper
- Within the sliding part of the zipper
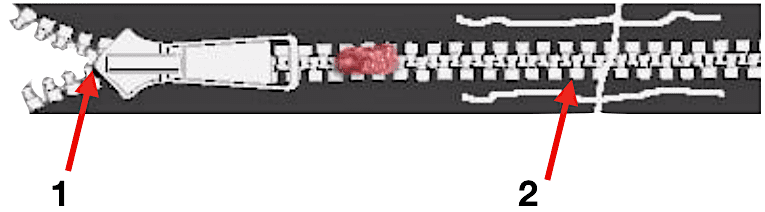
Entrapment involving the teeth of the zipper
This type of entrapment is easy to manage, and can often be accomplished without sedation or local anaesthesia. The zipper is cut horizontally above (1) or below (2) the site of entrapment and the teeth are gently pulled apart to release the foreskin.
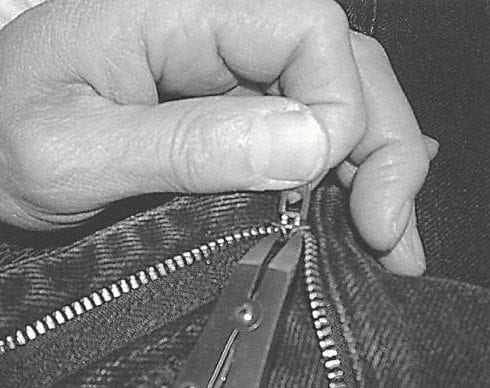
Entrapment involving the sliding part of the zipper
The sliding part of the zipper consists of anterior and posterior faceplates, connected by a small bridge called the median bar (or ‘diamond’). Entrapments here are released by cutting the median bar. This allows the anterior and posterior faceplates to fall apart, releasing the entrapped skin. The median bar can be cut with bone cutters, wire cutters or a mini-hacksaw.
An alternative technique involves placing the head of a small flathead screwdriver between the anterior and posterior faceplates and then rotating it 90 degrees to prise the faceplates apart. This widens the gap between the faceplates, releasing the skin.
Other techniques that have been suggested include:
- Soaking the penis in mineral oil for 10-15 minutes and then using gentle traction to slowly free the foreskin.
- Unzipping the zipper back over the entrapped skin (after infiltration of local anaesthetic)
- Applying lateral traction to the zipper teeth to pull them apart
The latter two techniques may cause further trauma to the penis and would not be recommended as an initial management strategy.
Finally, when all else fails, the penis can be freed using an elliptical skin incision or emergency circumcision (best performed by a urologist in the operating theatre under general anaesthesia).
Q3. What happened?
Show case outcome
Our patient had a large ‘bite’ of foreskin firmly wedged within the sliding part of the zipper. We used a pair of wire cutters to cut through the median bar.
This was a slow and difficult procedure: the median bar was bulky and the blades of the wire cutters were too broad, so we could not get them deep enough within the mechanism to completely encircle the bar. The median bar was finally cleaved by cutting obliquely with one blade of the wire cutters within the mechanism and the other blade resting outside it.
Despite the relatively long extraction time, the intranasal fentanyl and nitrous oxide provided good analgesia and amnesia – the patient had no recollection of the procedure whatsoever.
I definitely recommend investing in a pair of long, narrow-nosed wire cutters for this purpose, as broader-bladed tools may be too bulky to fit inside the mechanism and grasp the median bar.
References
- Flowerdew, R, Fishman, IJ, Churchill, BM. Management of penile zipper injury. J Urol 1977; 117:671. PMID: 859209
- Kanegaye, JT, Schonfeld, N. Penile zipper entrapment: a simple and less threatening approach using mineral oil. Pediatr Emerg Care 1993; 9:90. PMID: 8483788
- Nakagawa T, Toguri, AG. Penile Zipper Injury. Medical Principles and Practice 2006; 15: 303-304. PMID: 16763399
- Nolan, JF, Stillwell, TJ, Sands, JP. Acute management of the zipper-entrapped penis. J Emerg Med 1990; 8:305. PMID: 2373840
- Oosterlinck, W. Unbloody management of penile zipper injury. Eur Urol 1981; 7:365. PMID: 7286006
- Raveenthiran, V. Releasing of zipper-entrapped foreskin: a novel nonsurgical technique. Pediatr Emerg Care 2007; 23:463. PMID: 17666927
- Strait, RT. A novel method for removal of penile zipper entrapment. Pediatr Emerg Care 1999; 15:412. PMID: 10608329
- Wyatt, JP, Scobie, WG. The management of penile zip entrapment in children. Injury 1994; 25:59. PMID: 8132314
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |