
![]()
Ultrasound Case 017
Presentation
A 23 year old woman presents with right sided pelvic pain and vaginal spotting. Her last period was 6 or 7 weeks ago and her urinary BHCG is positive. You perform a transvaginal ultrasound.
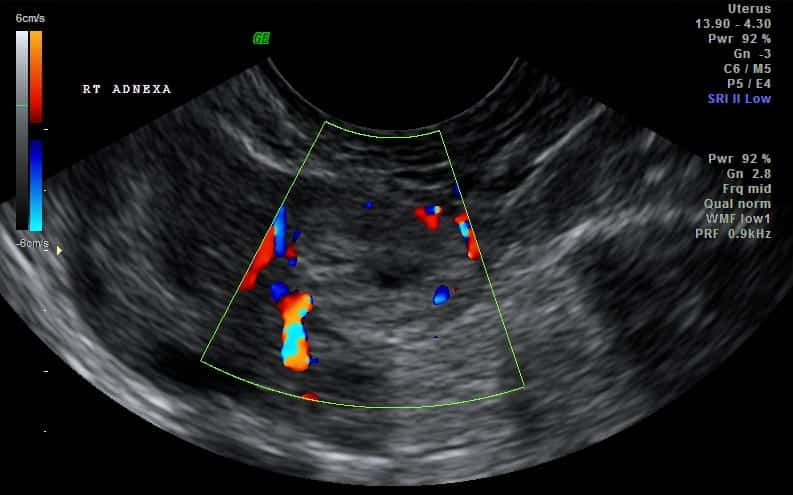
View 2 – Right adnexa
View 3 – Uterus

Describe and interpret these scans
IMAGE INTERPRETATION
Image 1: Transvaginal ultrasound, right adnexa, with intermittent gentle probe pressure.
The ovary is seen toward the left of the screen and contains a corpus luteum. In the centre of the image and directly abutting the ovary is a more echogenic ring shaped structure with hypoecheoic centre – the donut sign. This is typical of a small tubal ectopic – although a corpus luteum can appear identical. In order to differentiate the two, probe pressure is used to see if the two rounded structures move independently, sliding passed each other, or whether they move together as one indicating they are both likely to originate from the ovary.
Here independent movement is seen and the diagnosis of tubal ectopic is made.
Image 2: Colour Doppler does not help in differentiating a corpus luteum from an ectopic pregnancy as both may have a hypervascular surrounding ring – known as the ring of fire.
Image 3: The empty anteverted uterus.
CLINICAL CORRELATION
Tubal ectopic
Tubal ectopic pregnancies are common, occurring in about 1% of pregnancies. Bleeding and pain in early pregnancy provides a common diagnostic conundrum particularly when no definite intrauterine pregnancy is seen. The differential includes ectopic pregnancy, miscarriage, or early intrauterine pregnancy.
Assessment is made by correlating the clinical picture, the ultrasound findings and the quantitative BHCG. Only then can an appropriate and safe plan be made.
In this case a small round echogenic “donut” appearing adnexal mass with the typical features of an unruptured tubal ectopic is seen. The key task then is to determine whether the mass is indeed within the tube and separate from the ovary, or whether is is a corpus luteum and part of the ovary. Dynamic intermittent probe pressure as described above is key to sonographic assessment in this case and allowed us to proceed with definitive management.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |
Very good presentations!
Congratulations!