
![]()
IHD vs CRRT vs SLED
OVERVIEW
Continuous renal replacement therapy (CRRT) is the modality most widely used in Australia and New Zealand ICUs. There is no evidence suggesting mortality benefit for one modality over another (Cochrane Systemic Review)
Abbreviations:
- IHD = intermittent haemodialysis
- CRRT = continuous renal replacement therapy
- SLED = sustained low-efficiency dialysis or SLEDD = sustained low-efficiency daily dialysis
- VD = volume of distribution
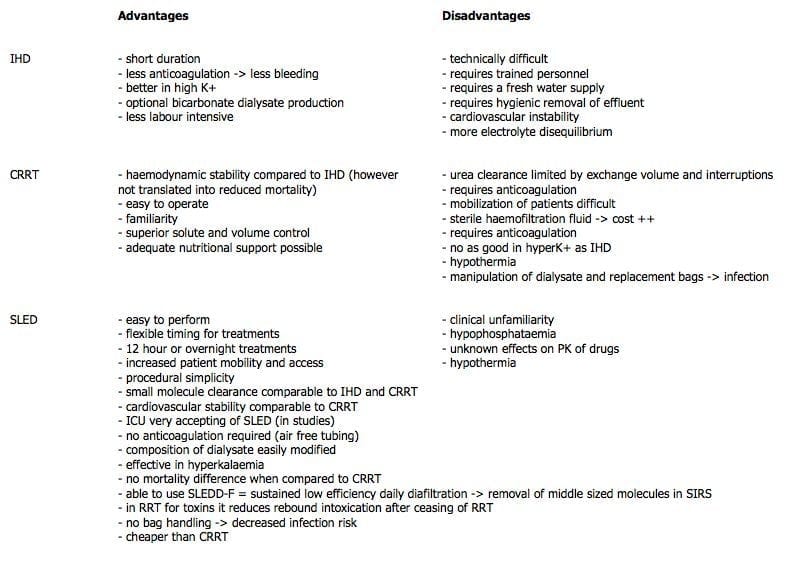
PROS AND CONS OF DIFFERENT MODALITIES
COMPARE AND CONTRAST DIFFERENT MODALITIES
| 1 | 2 | 3 | 4 |
|---|---|---|---|
IHD | SLEDD | CRRT | |
| Name | Intermittent hemodialysis | Slow (or sustained) low efficiency daily dialysis | Continuous renal replacement therapy |
| Mechanism and molecules removed | Dialysis – mostly low MWt | Small + middle molecules with SLEDD/F | Small + middle molecules with CVVHDF |
| Use |
|
|
|
| Blood flow | 300 - 400 mL/min | 100 - 150 mL/min | 150 - 200 mL/min |
| Dialysate flow |
|
|
|
| Efficiency | High | Moderate | Low (but increased clearance of high VD molecules over time) |
| Urea clearance (mL/min) | 150 | 80 | 30 (CVVHDF) |
| Hemodynamic stability | Poor (hypotension common) | Good | Good |
| Duration | 3-4 h 3x/week | 6-12 h daily | Continuous (24h/filter) |
| Access | Fistula or vascath (must be good!) | Fistula or vascath (must be good!) | Vascath only |
| Anticoagulation | Not needed | Usually not needed (if filter clots can lose ~150 mL blood) | Important (if filter clots can lose ~150 mL blood) |
| Dialysis Dysequilibrium Syndrome (DDS) | Insufficient time for equilibration between compartments can cause cerebral edema | N/A | N/A |
| Drugs and toxicology | Risk of rebound if high VD. Better for low VD (e.g. toxic alcohols) | Unclear effects on drug pharmacokinetics | Slower removal |
| Logistics | Need tap water supply, need hygienic effluent removal, Technically difficult | High start up costs, low familiarity, low running costs, Hypophosphatemia | High workload, clearance limited by interruptions, costly sterile dialysate bags, immobility |

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC