
![]()
Rendu-Osler-Weber disease
Description
Rendu-Osler-Weber disease (aka Hereditary haemorrhagic telangiectasia (HHT)) is an autosomal dominant disorder characterised by epistaxis, cutaneous telangiectasia, and visceral arteriovenous malformations (AVMs).
Characteristic lesions are telangiectases – focal dilatations of postcapillary venules and AVMs. Recurrent epistaxis often restricts daily life and AVMs can cause serious complications if located in the lungs, liver, or brain.
History
1864 – English physician, Henry Gawen Sutton (1837-1891) is oft cited as the original describer of the condition. His publication recounts recurrent sever epistaxis and haemoptysis with no attending cutaneous features described.
1865 – Benjamin Guy Babington (1794–1866), in a letter to the Lancet, provided a description of epistaxis in five generations of one family.
Thus epistaxis, violent and habitual, has been observed in five consecutive generations, and for the last three generations in two branches. I have myself at different times attended Mrs. K-, her two daughters, and her grandson, and in all the haemorrhage was on more than one occasion so violent as to necessitate the operation of plugging ; and in the cases of the daughters and grandson to give rise to the apprehension of a fatal result.
1876 – The English physician John Wickham Legg (1843-1921) read a paper before the Royal Medical and Chirurgical Society of London on a Case of Haemophilia complicated with Multiple Naevi. The patient, a musician, aged 65 years, had been subject to epistaxis from boyhood. He had numerous small naevi over the face, forehead, and various parts of the trunk which had been first noticed when he was about 41 years of age. Several members of his family suffered from epistaxis.
1896 – French physician, Henri Jules Louis Marie Rendu (1844-1902) published the case of a 52-year-old male who presented with epistaxis. He was well developed but pale and weak, with a subicteric tint. His father suffered from dysentery and repeated melena and died at 55 years of age; the mother and brother suffered from copious epistaxes.
He had his first nose bleeds at the age of 12 years, and throughout his youth he was subject to them, chiefly in the spring and in the warm season. This disposition, far from attenuating with advancing age, became considerably aggravated, and since the age of 35 the haemorrhages have become very frequent, always in the form of epistaxis.
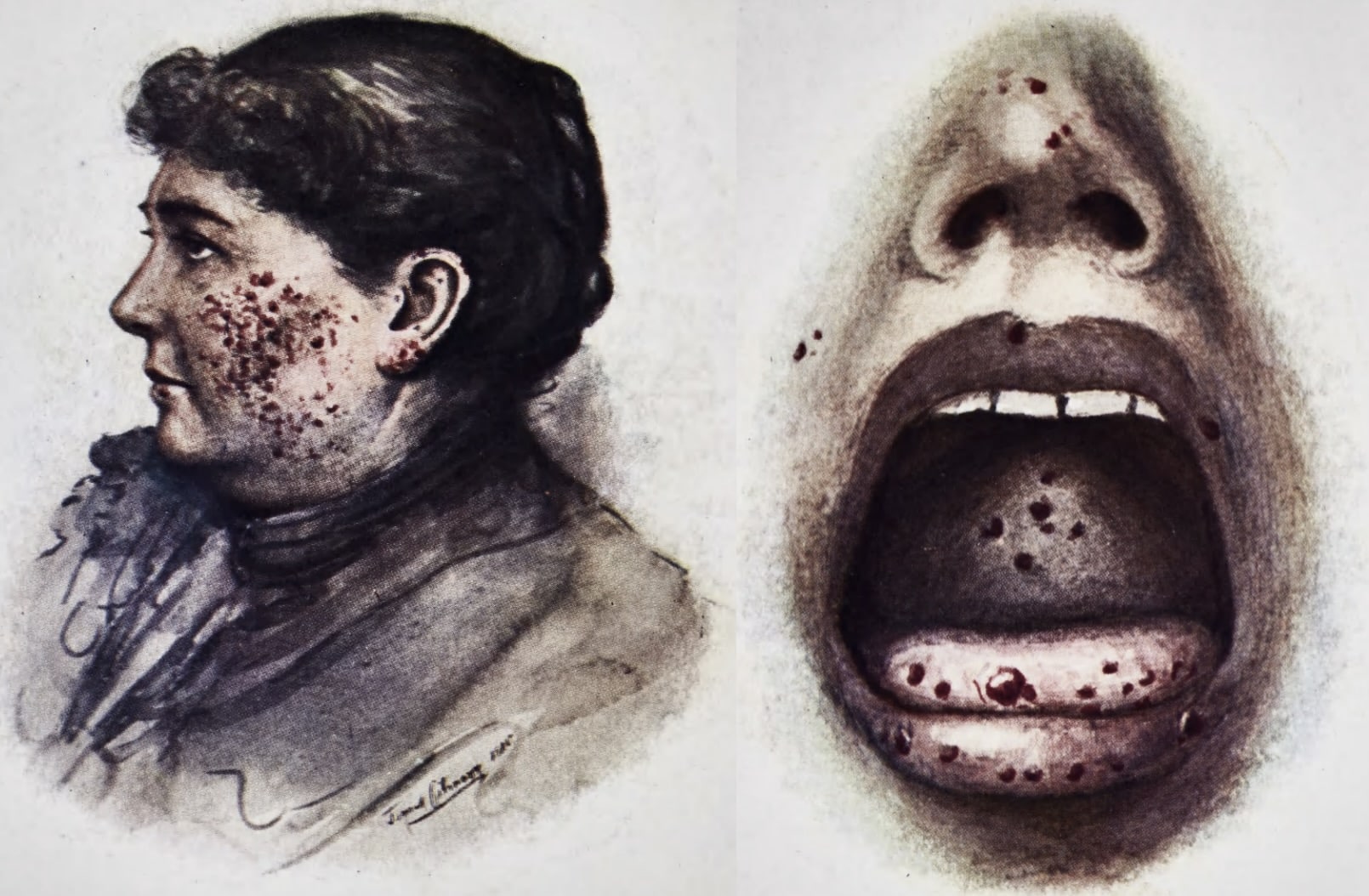
On the skin of the nose, the cheeks, the upper lip, and the chin, there are small purple spots as large as the head of a pin; the largest reach the size of a lentil; they are true cutaneous hemangiomas, produced by a dilatation of the superficial vessels of the skin. Pressure causes them to blanch, but not to disappear; the blood flows back immediately when compression is released.
Angiomas of the same nature are scattered over the neck and chest; there appear to be none on the extremities. This anatomic disposition is not limited to the skin; it extends also to the mucous membranes, and this fact is of considerable interest from the point of view which concerns us. Indeed, small vascular dilatations, true telangiectatic foci, are present on the inner surface of the lips and the cheeks, on the tongue, and on the soft palate, with characteristics identical to those on the integument, but with a very bright colour, owing to the decreased thickness of mucous epidermis. In the nostrils we have not demonstrated these punctiform angiomas, but it is not irrational to suppose that there are similar ones on the nasal septum or in the nasal mucous membrane that is the seat of the haemorrhages, and why they are so recurrent and copious.
1901 – Sir William Osler (1849-1919) published the first comprehensive description of Hereditary haemorrhagic telangiectasia (HHT), emphasising the familial nature of the condition.
In the three cases here described, two belonged to a family in which epistaxis had occurred in seven members. Both of my patients had had bleeding at the nose from childhood, and both presented numerous punctiform angiomata on the skin of the face and of the mucous membrane of the nose, lips, cheeks and tongue.
The third patient had suffered in an unusual degree from recurring epistaxis, and the telangiectases were most abundant over the body, and very numerous also on the mucous membranes. The condition has nothing to do with haemophilia, with which the cases had been confounded
In Case II, William B had suffered from epistaxis since childhood and died of gastric cancer. At autopsy
Osler noted that the viscera could be affected “In the stomach there were a dozen round foci, each 3 to 4 mm. in size, which at first looked like ecchymoses but were dilated venules and capillaries.”
1906 – Adam Brown Kelly (1866-1941) presented two sisters, aged 40 and 41 years. Their father had been subject to attacks of epistaxis, had facial ‘spots’ similar to their own, and died aged 62 in consequence of frequent bleedings from the nose. The elder of the two sisters died suddenly from syncope induced by severe epistaxis. A daughter (aged 23 years) had also developed telangiectasis on her face. In Brown Kelly’s patients, the telangiectasis developed later in life.
1907 – Frederick Parkes Weber (1863-1972) provided a clinical description in a series of cases; and provided a summary of the world literature to date. He would later exand further with more cases in 1936
Mrs. Sarah S…has a number of bright red angiomata distributed over the face, ears, lips, tongue, mucous membrane of the mouth, and the conjunctival surfaces of the four eyelids. All these angiomata are small; many, including those on the tongue and inside of the mouth, are hardly as large as an ordinary brass pin’s head (punctiform angiomata)
On the mucous membrane inside both nostrils there are some telangiectases…On the fingers, and notably under the finger-nails, there are several minute (pinpoint) red angiomata, which I had not observed until Professor W. Osler, when he recently saw the patient, kindly drew my attention to them.

Associated Persons
- Henry Gawen Sutton (1837-1891)
- Benjamin Guy Babington (1794-1866
- Henri Jules Louis Marie Rendu (1844-1902)
- Sir William Osler (1849-1919)
- Adam Brown Kelly (1866-1941)
- Frederick Parkes Weber (1863-1972)
Alternative names
- Hereditary haemorrhagic telangiectasia (HHT)
References
Historical references
- Sutton HG. Epistaxis as an indication of impaired nutrition, and of degeneration of the vascular system. Medical Mirror (London) 1864; 1: 769-781
- Babington BG. Hereditary epistaxis. Lancet 1865; 86(2195): 362-363
- Legg JW. A case of haemophilia complicated with multiple naevi. Lancet 1876; 108(2781): 856-858
- Rendu H. Epistaxis répétés chez un sujet porteur de petits angiomes cutanés et muqueux.
Gazette des hôpitaux civils et militaires (Lancette française) 1896; 69: 1322-1323. - Osler WB. On a family form of recurring epistaxis, associated with multiple telangiectases of the skin and mucous membranes. Bulletin of the Johns Hopkins Hospital. 1901; 12(128): 333-337.
- Kelly AB. Multiple Telangiectases of the Skin and Mucous Membranes of the Nose and Mouth. Glasgow Med J. 1906 Jun;65(6):411-422.
- Weber FP. Multiple hereditary developmental angiomata (telangiectases) of the skin and mucous membranes associated with recurring haemorrhages. Lancet 1907; 170(4377): 160-162
- Weber FP. Haemorrhagic telangiectasia of the Osler-type «telangiectatic dysplasia» and isolated case, with discussion on multiple pulsating stellate telangiectases and other striking haemangiectatic conditions. British Journal of Dermatology. 1936; 48(4): 182-193.
Eponymous term review
- Henri Rendu (1844-1902). Rendu-Osler-Weber disease. JAMA. 1966 Aug 15;197(7):583.
- Fuchizaki U, Miyamori H, Kitagawa S, Kaneko S, Kobayashi K. Hereditary haemorrhagic telangiectasia (Rendu-Osler-Weber disease). Lancet. 2003 Nov 1;362(9394):1490-4.
eponymictionary
the names behind the name