
![]()
A Lesson in History
aka Gastrointestinal Gutwrencher 003
A 28 year old man, originally from Somalia, presents to the emergency department having been unwell for the past week or so. He complains of poor appetite and tiredness, and is particularly concerned that his eyes have turned yellow. On examination he has icteric sclera and a tippable mildly tender liver.
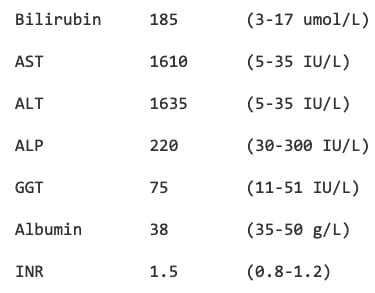
His ‘LFTs’ (with reference ranges) are:
Questions
Q1. Describe the LFTs.
Answer and interpretation
There is hyperbilirubinemia and markedly raised ALT/AST (“transaminitis”), with relatively normal ALP and GGT. This is suggestive of a ‘hepatocellular’ or ‘hepatitic’ picture, rather than a cholestatic picture. The elevated INR of 1.5 is consistent with liver synthetic dysfunction.
Overall, this suggests liver failure due to hepatitis.
Q2. What causes need to be considered?
Answer and interpretation
Important causes of hepatitis include the following (although some, such as hepatitis A, do not result in liver failure):
- viruses — Hepatitis virues A to E; HSV, EBV, CMV
- drugs and toxins — e.g. paracetamol, halothane, isoniazid, Amanita mushrooms, herbal medicines.
- alcoholic hepatitis
- non-alcoholic steatohepatitis and acute fatty liver of pregnancy (unlikely in this case!)
- ischemic hepatitis, veno-occlusive disease and Budd-Chiari syndrome
- autoimmune hepatitis
An exhaustive search, involving numerous investigations, for the above causes was fruitless. Furthermore, the patient denies any of the usual risk factors for hepatitis (e.g. drug use, risky sexual practices, tattoos, blood transfusions etc.), does not drink alcohol and has not left Australia for 15 years. He denies taking any medications and has no significant past medical problems. However, he has been in contact with another Somalian who also had yellow eyes.
Q3. What question should you specifically ask a person from East Africa or the Middle East who presents with an LFT profile similar to this?
Answer and interpretation
“Do you use khat?”
The chewing of khat leaves (Catha edulis) is a widespread recreational custom in East Africa and the Arabian Peninsula. Leaves are chewed for several minutes and then placed into the cheek as the juice is slowly swallowed. The plant contains the alkaloids cathine and cathinone, which have amphetamine-like stimulant properties.
The use of khat may not be considered a drug or a herbal medicine by the patient.

Q4. Why is this important?
Answer and interpretation
The toxic effects of khat include:
- sympathomimetic effects due to increased release of dopamine and other neurotransmitters from presynaptic neuronal storage.
- overdose may result in:
- psychosis with visual hallucinations and mania
- rhabdomyolysis
- cardiac dysrhythmias
- stroke
- altered sensorium
- convulsions
- chronic use may result in:
- myocardial infarction and ischemic cardiomyopathy
- strokes
- oral carcinomas
- hepatitis (acute or chronic)
That’s right, hepatitis.
Repeated use of khat may result in multiple episodes of subclinical hepatitis, eventually resulting in chronic liver disease. However, acute severe hepatotoxicity can occur even in the absence of chronic liver disease. A high concentration of cathionine may be detected in liver tissue at biopsy.
Q5. What is the prognosis?
Answer and interpretation
Patients with khat-induced hepatoxicity may develop acute liver failure due to multilobar necrosis. This may ultimately require liver transplantation, or failing that, result in death.
The person that this case-based Q&A was inspired by ultimately received a liver transplant.
References
- Auerbach P, Wilderness Medicine (5th Edition), Mosby Elsevier 2007 [mdconsult.com]
- Chapman MH, Kajihara M, Borges G, O’Beirne J, Patch D, Dhillon AP, Crozier A, Morgan MY. Severe, acute liver injury and khat leaves. N Engl J Med. 2010 Apr 29;362(17):1642-4. PMID: 20427816. [fulltext]
CLINICAL CASES
Gastrointestinal Gutwrencher
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
