
![]()
Above the Ears
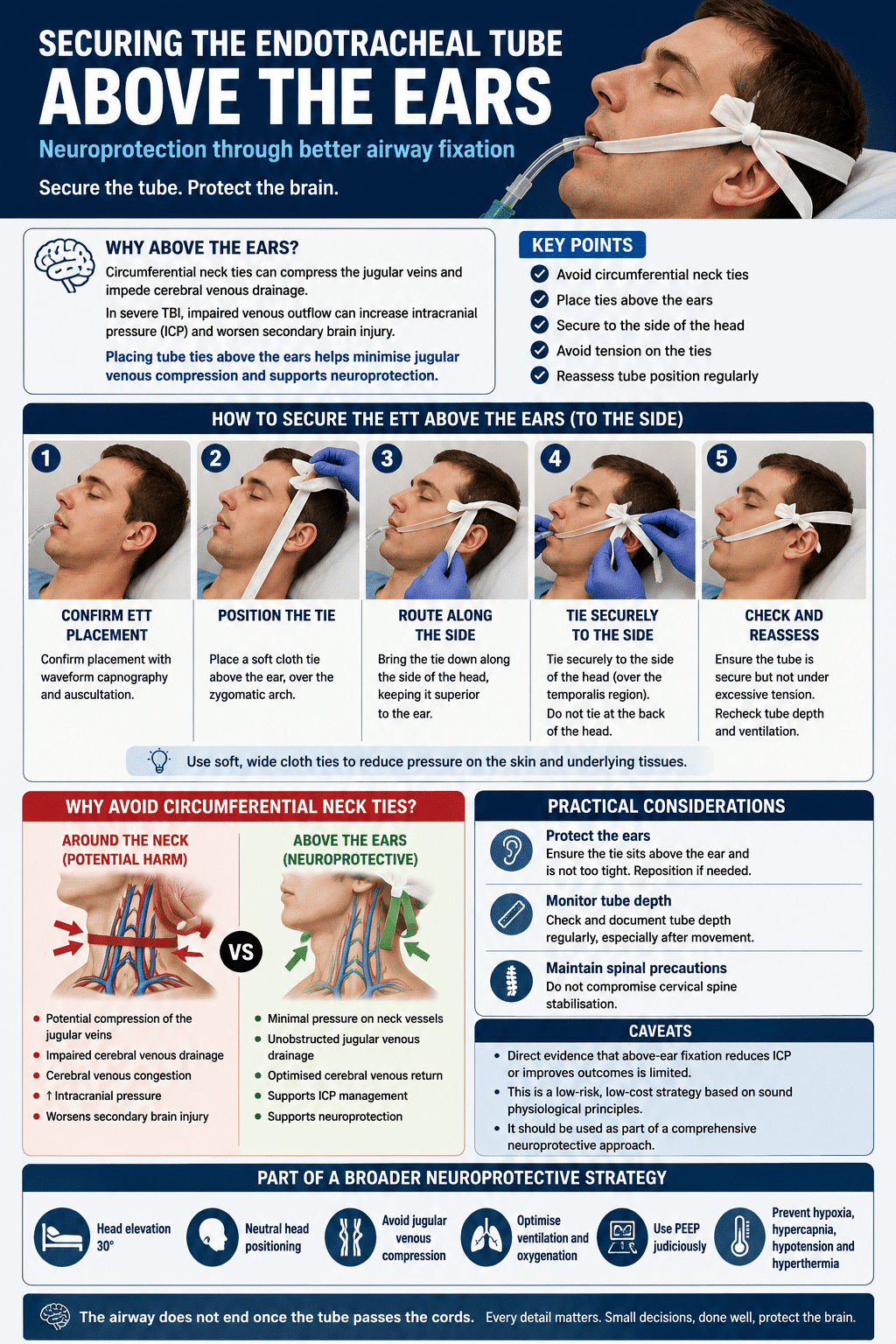
Securing the endotracheal tube (ETT) for neuroprotection
The airway does not end once the tube passes the cords
Case: A 28-year-old male is brought to the Emergency Department after a high-speed motorcycle collision. He is combative, confused, and vomiting. Initial observations reveal:
- GCS 7 (E1 V2 M4)
- Unequal pupils
- Hypertension and bradycardia
- Bleeding from the scalp and face
- Oxygen saturations are falling despite high-flow oxygen
Rapid sequence intubation is performed for airway protection and anticipated neurological deterioration. Following confirmation of tube placement, attention turns to securing the ETT.
Instead of passing tube ties circumferentially around the neck, the airway team secures the tube using cloth ties positioned superiorly above the ears and around the occiput while preparing for rapid transport to the CT scanner.

Why above the ears? What is the neurophsiology behind it?
The cranial vault is a fixed space governed by the Monro–Kellie Doctrine. Brain tissue, blood, and cerebrospinal fluid coexist within a rigid skull. When one component increases, another must decrease to prevent intracranial pressure rising.
In severe traumatic brain injury:
- Cerebral oedema develops
- Venous congestion worsens
- Autoregulation may fail
- Small increases in venous pressure can significantly increase ICP
Anything that impedes cerebral venous outflow may worsen secondary brain injury.
Circumferential neck ties can theoretically:
- Compress the jugular veins
- Increase cerebral venous congestion
- Impair venous drainage from the brain
- Contribute to elevated ICP
This is particularly relevant in patients with:
- Severe TBI
- Cerebral oedema
- Intracranial haemorrhage
- Raised ICP
Why not just tape the tube as intensive care does?
Airway management and resuscitation in the pre-hospital or emergency department settings often occur under time-critical and at times chaotic conditions. In general the intensive care unit or operating theatre provides for a more controlled environment. Head-injured patients are frequently diaphoretic, contaminated with blood or vomitus, immobilised in cervical collars or head blocks. In this setting, adhesive tape fixation of the endotracheal tube can be unreliable and prone to loosening or dislodgement, particularly during repeated patient handling and movement to CT.
The priority during the initial resuscitation phase is rapid stabilisation, neuroprotection, and safe transfer rather than meticulous tape fixation. Cloth tie fixation above the ears in neurotrauma patients provides rapid, secure airway stabilisation in difficult conditions.
Definitive adhesive taping or commercial fixation devices can then be applied later in a more controlled environment, such as ICU or theatre, once the patient is stabilised and facial contamination has been addressed.
The practical approach
A simple approach to securing the ETT involves:
- Confirm ETT placement
- Apply soft cloth tube ties
- Place ties superiorly over the zygomatic arch, then over the ears
- Secure behind the occiput rather than around the neck
- Ensure adequate fixation without excessive tension
Care must still be taken to:
- Prevent tube migration
- Avoid pressure injuries to the ears
- Frequently reassess tube depth
- Maintain cervical spine precautions if required
Caveats and review of the evidence
The rationale for avoiding circumferential neck ties in severe neurotrauma is supported by the principles described in the non-fatal strangulation literature. Studies examining neck compression show that even small amounts of external pressure can impair venous and arterial flow within the neck. Occlusion may occur with forces well below what an adult hand can easily generate. For example jugular venous occlusion with 4 psi of external pressure and carotid artery compression with 11 psi of external pressure
Venous obstruction occurs before arterial compromise, resulting in cerebral venous congestion and rising intracranial pressure before any significant reduction in arterial inflow. Although ETT ties are not equivalent to strangulation, the principle is still relevant in the severely head-injured patient. Cerebral venous drainage may already be impaired by cerebral oedema, cervical collars, suboptimal positioning, and positive pressure ventilation.
In the environment of emergency airway management, additional neck compression from circumferential tube ties may represent another potentially avoidable contributor to impaired cerebral venous outflow. Avoiding tight neck fixation and placing ties above the ears represents a simple, low-cost neuroprotective strategy aimed at minimising resistance to jugular venous drainage during the early resuscitation phase.
There is limited direct evidence proving that above-ear fixation reduces intracranial pressure or improves neurological outcomes. The concept should still sit within the broader neuroprotective strategies aimed at optimising cerebral venous return such as:
- Head elevation to 30 degrees
- Neutral neck positioning
- Avoidance of jugular venous compression
- Judicious use of PEEP when appropriate
- Careful cervical spine precaution management
References
- Seyedhosseini J, Ahmadi M, Nejati A, Ardalan A, Ghafari M, Vahidi E. Two Different Endotracheal Tube Securing Techniques: Fixing Bandage vs. Adhesive Tape. Adv J Emerg Med. 2017 Oct 13;1(1):e3.
- Singh G, Manikandan S, Neema PK. Endotracheal tube fixation in neurosurgical procedures operated in prone position. J Anaesthesiol Clin Pharmacol. 2011 Oct;27(4):574-5.
- De Boos J. Review article: Non-fatal strangulation: Hidden injuries, hidden risks. Emerg Med Australas. 2019 Jun;31(3):302-308.
- Preparation for Retrieval. Trauma Victoria
Emergency Procedures
Emergency nurse with ultra-keen interest in the realms of toxicology, sepsis, eLearning and the management of critical care in the Emergency Department | LinkedIn |