
![]()
Adie syndrome
Holmes-Adie syndrome (Adie syndrome) is a benign, typically unilateral neurological condition characterised by a tonic pupil, light–near dissociation, and absent deep tendon reflexes.
It results from postganglionic parasympathetic denervation, most commonly at the level of the ciliary ganglion, and may also affect autonomic fibres to spinal reflex arcs.
Unilateral tonic pupil is more common in women, often presenting in early adulthood. While typically idiopathic, associations with viral or bacterial illness, trauma, or autoimmune disorders have been documented.
Clinical Features
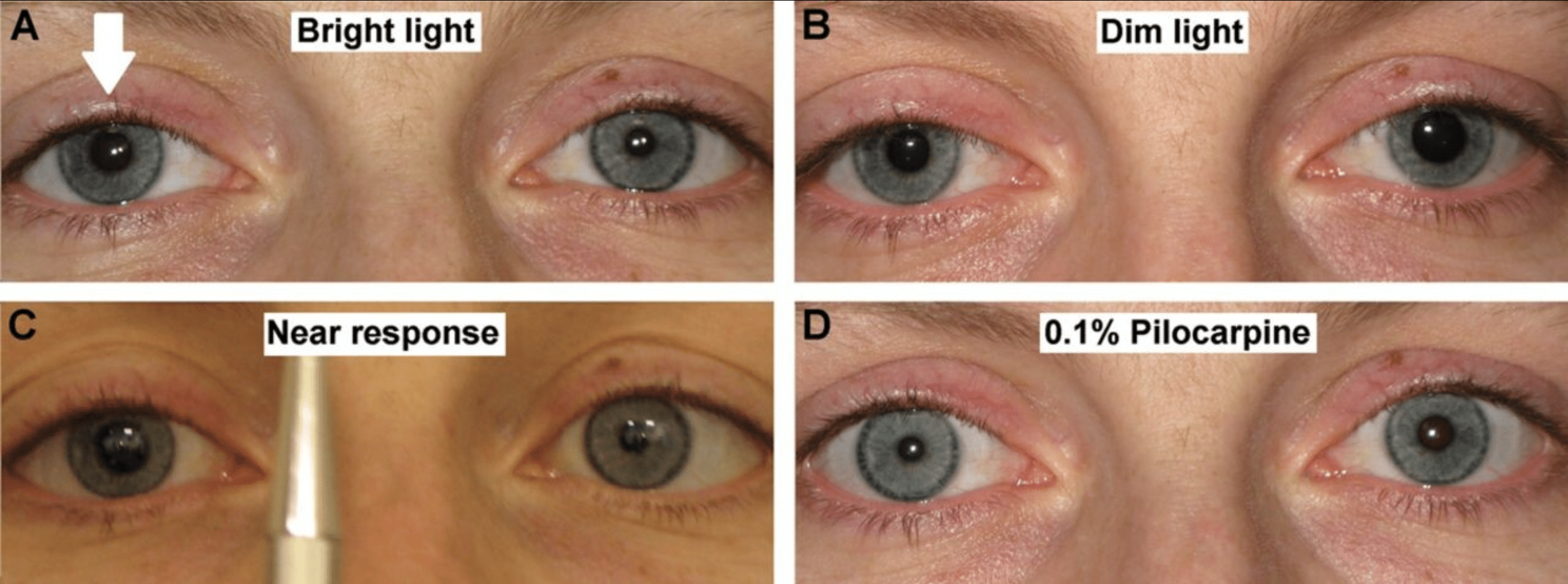
- Tonic pupil: Unilaterally enlarged pupil with poor or absent light reaction but a slow, sustained constriction to near effort (light–near dissociation), followed by delayed redilation.
- Light–near dissociation (LND): Pupils that do not respond (or respond poorly) to light but constrict appropriately (albeit slowly) with accommodation.
- Absent deep tendon reflexes: Most often Achilles; sometimes patellar.
- Accommodation lag, photophobia, blurry near vision are common symptoms.
- Often identified incidentally or after a mild viral illness.
Investigations
- Pilocarpine 0.125% test: Hypersensitivity to dilute pilocarpine confirms postganglionic denervation, the tonic pupil will constrict markedly due to cholinergic supersensitivity.
- Neuroimaging or labs may be used to exclude structural or infectious causes, but often unnecessary in classic cases.
Terminology Notes
- Adie’s pupil: Refers to the tonic pupil alone.
- Holmes–Adie syndrome or Adie syndrome: Describes the combined presentation of tonic pupil and areflexia.
- Incomplete forms may feature only pupil or reflex changes.
- May overlap with broader autonomic neuropathies, including variants involving sweating or cardiovascular reflex abnormalities.
History of Holmes-Adie syndrome
1812 – James Ware in his dissertation on Observations relative to the near and distant sight of different persons describes a woman with longstanding unilateral mydriasis and light-near dissociation:
A lady between thirty and forty years of age, the pupil of whose right eye, when she is not engaged in reading, orin working with her needle, is always dilated very nearly to the rim of the cornea; but whenever she looks at a small object, nine inches from the eye, it contracts…Her left pupil is not affected like the right
Ware 1812
1881 – John Hughlings Jackson (1835–1911) presented a detailed case of a healthy 26-year-old woman with a unilateral dilated tonic pupil, unresponsive to light but with preserved accommodation, and absent knee-jerk reflexes with no other neurological findings in Transactions of the Ophthalmological Society of the United Kingdom
The right pupil was dilated and absolutely motionless to light, and also during accommodation, yet the accommodation itself on this side was perfect… Neither I nor Mr. Couper found the smallest trace of the knee phenomenon… she is seemingly in perfect health.
Hughlings Jackson 1881
This is arguably the earliest full clinical description of Holmes–Adie syndrome presenting a tonic pupil with areflexia in an otherwise well patient.
1902 – Neurologisches Centralblatt publishes four landmark papers on myotonic pupils, each offering observations on abnormal pupillary movements now recognised as features of tonic pupils.
- Julius Strassburger (1871-1934) Described “pupillary sluggishness with accommodation and convergence” (Pupillenträgheit), noting that in some patients, the pupil was “slow or absent to light but reactive to near effort.” His work underscored the dissociation between light and near responses, a defining feature of the Adie pupil. [21(16): 738–740]
- Alfred Saenger (1860-1921) Introduced the term “myotonische Pupillenbewegung”, describing: “Langsame Kontraktion und sehr verlangsamte Dilatation bei Konvergenz… eine Bewegung wie bei Myotonie.” (Slow contraction and even slower dilation during convergence… a movement akin to myotonia). His analogy to myotonia highlighted the neuromuscular-like sluggishness of the iris sphincter. [21(18): 837-839]
- Max Nonne (1861-1959) confirmed the key findings of light–near dissociation and tonic pupil behaviour. Argued that “myotonic” was a misnomer and that the delayed pupil reaction was neurological, not muscular in origin [21(21): 1000-1004]
- Saenger published Über die Bezeichnung “myotonische Pupillenbewegung” defending and clarifying the use of “myotonic” to describe the phenomenon, responding to Nonne’s criticisms.
Together, these papers provided a cohesive description of the tonic pupil; introduced the concept of light–near dissociation (LND); and framed an early debate on nomenclature that predated Adie by nearly 30 years.
1905 – Charles Markus (1874–1958) presented a patient with a dilated, tonic pupil and absent knee and ankle jerks to the Ophthalmological Society of the UK in 1905, published in 1906 as “Notes on a Peculiar Pupil Phenomenon in a Case of Partial Iridoplegia”, he described:
The right pupil was widely dilated to a diameter of 8 mm… it contracted slowly on accommodation… and took about four minutes to return to its original size. There were no knee-jerks or heel-jerks
Markus 1906
This was the first description in English medical literature of a tonic pupil associated with absent deep tendon reflexes. The case was reviewed 27 years later by Frederick Parkes Weber (1863-1972) who confirmed stable, benign findings. Writing in 1942, Markus reaffirmed:
The tonic pupil is described for the first time in English medical literature… associated with absence of the knee jerks. This was the first observation of its kind
Markus 1942
1914 – Hans Oloff published Ueber die myotonische Konvergenzreaktion der Pupille describing two cases of myotonic convergence reaction. Oloff noted prolonged pupillary constriction after convergence, slow or absent light reaction, and absent patellar reflexes.
Von Augensymptomen ist beiden Fällen gemeinsam das Vorhandensein… einer einseitigen myotonischen Konvergenzreaktion bei aufgehobener bzw. fast aufgehobener Lichtreaktion dieser Seite.
Oloff 1914
Both cases shared… a unilateral myotonic convergence reaction with absent or nearly absent light reaction on that side.
He differentiated the condition from syphilitic origins citing negative Wassermann and cerebrospinal fluid findings in both patients, countering misdiagnoses of neurosyphilis. This added to growing evidence of clinical differentiation from Argyll Robertson pupil.
1926 – Georges Weill (1866-1952) and Louis Reys summarised the condition in French describing tonic (myotonic) pupil with convergence-provoked constriction, accommodative paresis, lack of light response, and absent lower limb reflexes. They emphasized a combined cerebrospinal and sympathetic pathogenesis, suggesting a broader autonomic disorder (“…il y aurait association de troubles cerebrospinaux et sympathiques…”).
1931 – William John Adie (1886-1935) described six cases of patients (five women) with tonic pupils and areflexia, without evidence of syphilis in Pseudo-Argyll Robertson Pupils with Absent Tendon Reflexes: A Benign Disorder Simulating Tabes Dorsalis. Adie emphasised the benign nature of the disorder and its frequent misdiagnosis as neurosyphilis
I wish to draw attention to a benign symptomless disorder characterized by pupils which react on accommodation but not to light, and by absent tendon reflexes…Though harmless in itself it merits recognition because it is often mistaken for a manifestation of syphilis of the nervous system, with unfortunate consequences…
Adie, May 1931
Adie recognised the work of his colleagues including Symonds, Holmes, Markus and Robert Foster Moore (1878-1963) who later expressed his ‘dissatisfaction’ at not having been ascribed the eponym…
Note – After this was written, Mr. Foster Moore kindly allowed me to read the typescript of his paper on the non-luetic Argyll Robertson pupil, which he read at the recent ophthalmological congress. In one of his fifteen patients with this abnormal reaction of the pupil, the knee-jerks were absent: in another they were obtained with reinforcement only.
1931 – Gordon Morgan Holmes identified 19 patients with myotonic pupils and presented his paper Partial iridoplegia to the Ophthalmological Society of the United Kingdom
By very slow contraction on convergence, and even slower relaxation. The reflex to light is often lost too. One or both eyes may be affected.… In the present state of our knowledge a separation of those cases in which the tendon jerks are absent from those in which they persist is unjustifiable…the similarity of the symptoms in all these cases naturally suggests a common aetiology.
Holmes, 1931
1932 – Adie publishes a definitive review of tonic pupils and absent reflexes, formally describing the syndrome as “a benign disorder sui generis.” In Tonic pupils and absent tendon reflexes, Adie consolidated his clinical observations with long-term follow-up. He presented 19 personal cases and reviewed 45 others from literature, noting that many had been misdiagnosed with tabes dorsalis.
This benign disorder, sui generis, seems to me to be distinct from all known organic diseases of the nervous system… it does not progress, has no grave underlying cause, and does not indicate syphilis.
Adie, 1932
Adie divided the condition into complete and incomplete forms, depending on whether tendon reflexes were also absent. This work definitively established the syndrome’s identity, epidemiology, and long-term benign course.
1933 – Frederick Parkes Weber (1863-1972) re-examined the original 1905 patient of Charles Markus, documenting persistent tonic pupil and areflexia nearly three decades later. This long-term follow-up supported the benign nature of the condition later defined by Adie. Weber wrote:
The patellar and Achilles reflexes are still absent, and the right pupil is still of the ‘myotonic’ type… He has continued to enjoy good health; he can work well, and is married and has two healthy children.
Weber 1933
1932 – Georges Guillain and Jean Édouard Sigwald (1903–1975) published Sur une affection spéciale non syphilitique caractérisée par des troubles pupillaires et l’abolition des réflexes tendineux, and first applied the term “maladie d’Adie” to describe nonsyphilitic tonic pupil–areflexia syndrome
1934 – Jean-Alexandre Barré (1880-1967) used the term ‘syndrome d’Adie‘. He acknowledged the prior descriptions by Weill & Reys and others but argued for naming the condition after the clinician who best defined its clinical identity and benign nature: Adie
1936 – Edwin Bramwell (1873–1952) formally proposes the eponym “Holmes-Adie Syndrome” at the March meeting of the Medico-Chirurgical Society of Edinburgh. Noting the condition’s frequent misdiagnosis as tabes dorsalis or neurosyphilis, he advocated naming the syndrome to improve recognition.
Bramwell synthesised the published work of Holmes and Adie, highlighting the shared features: tonic pupil(s), often unilateral; absent deep tendon reflexes; and benign, non-syphilitic progression. He wrote:
I propose to suggest that it be known as the Holmes-Adie syndrome, and will give reasons which appear to me to justify this designation.
The Holmes-Adie syndrome is a relatively not uncommon clinical entity…characterised…by pupils…immobile or very defective in their response to light…show[ing] the tonic reaction—a delayed, slow, and extreme contraction with still slower dilatation… and by diminution or loss of some of the deep reflexes
Bramwell, 1936
Alternative names
- Adie pupil
- Adie-Holmes syndrome
- Holmes-Adie syndrome
- Weill-Reys syndrome
- Markus syndrome
Associated Persons
- James Ware (1756-1815)
- John Hughlings Jackson (1835-1911)
- William John Adie (1886-1935)
- Gordon Morgan Holmes (1876-1965)
- Jean-Alexandre Barré (1880-1967)
References
Original articles
- Ware J. Observations relative to the near and distant sight of different persons. Philosophical Transactions of the Royal Society of London, 1813: 103: 31–50.
- Hughlings Jackson J. VIII: Paralytic affections. In: Transactions of the Ophthalmological Societies of the United Kingdom, 1881; 1: 139-154.
- Strassburger J. Pupillenträgheit bei Accommodation und Convergenz. Neurologisches Centralblatt 1902; 21(16): 738-740
- Saenger A. Über myotonische Pupillenbewegung. Neurologisches Centralblatt 1902; 21(18): 837-839
- Nonne M. Über die sogenannte “myotonische” Convergenzträgheit lichstarrer Pupillen. Neurologisches Centralblatt, 1902; 21(21): 1000-1004
- Saenger A. Über die beziechung “myotonische Pupillenbewegung. Neurologisches Centralblatt, 1902; 21(24): 1137-1138
- Markus C. Notes on a Peculiar Pupil Phenomenon in a Case of Partial Iridoplegia, Transactions of the Ophthalmological Society of the United Kingdom 1906; 26: 50-58
- Oloff H. Ueber die myotonische Konvergenzreaktion der Pupille. Klinische Monatsblätter für Augenheilkunde. 1914; 53: 493-502.
- Foster Moore R. Discussion on Physiology and Pathology of the Pupil reactions. Transactions of the Ophthalmological Society of the United Kingdom 1924; 44: 38
- Weill G, Reys L. Sur la pupillotonie. Contribution a l’étude de sa pathogénie. A propos d’un cas de réaction tonique d’une pupille a la convergence et parésie de l’accommodation avec aréflexie a la lumière chez un sujet atteint de crises tétaniformes et d’aréflexie des membres inférieurs. Revue d’oto-neuro-oculistique, Paris, 1926; 4: 433-441.
- Holmes G. Partial iridoplegia associated with symptoms of other diseases of the nervous system. Transactions of the Ophthalmological Society of the United Kingdom 1931; 51: 209-28
- Adie WJ. Pseudo-Argyll Robertson pupils with absent tendon reflexes. A benign disorder simulating tabes dorsalis. Br Med J. 1931; 1(3673): 928-30.
- Adie WJ. Argyll Robertson pupils true and false Br Med J. 1931; 2(3681): 136-8.
- Adie WJ. Tonic pupils and absent tendon reflexes: a benign disorder sui generis; its complete and incomplete forms. Brain 1932; 55: 98–113
- Adie WJ. Complete and incomplete forms of the benign disorder characterised by tonic pupils and absent tendon reflexes. Br J Ophthalmol. 1932 Aug;16(8):449-61.
- Guillain G, Sigwald J. Sur une affection spéciale non syphilitique caractérisée par des troubles pupillaires et l’abolition des réflexes tendineux. Bulletins et Mémoires de la Société médicale des hôpitaux de Paris 1932 [maladie d’Adie]
- Weber FP. Dr. Markus’s Original Case of Markus’s Syndrome (“Myotonic Pupil” with Absence of Patellar and Achilles Reflexes) shown twenty-seven and a half years ago. Proc R Soc Med. 1933 Mar;26(5):530-1.
- Barré JA, Klein M. Etude d’un cas de syndrome d’Adie. Revue neurologique 1934: 590 [syndrome d’Adie]
- Bramwell E. The Holmes-Adie Syndrome: A Benign Clinical Entity Which Simulates Syphilis of the Nervous System. Edinb Med J. 1936 Jun;43(6):T83-T92.
Review articles
- Leprat S. Contribution à l’étude du syndrome de Weill-Reys (alias Syndrome d’Adie). 1941
- Markus C. The tonic pupil. Br J Ophthalmol. 1942 Mar;26(3):137-8.
- Dynes JB. Adie’s syndrome: its recognition and importance. JAMA. 1942;119(18):1495-1497
- Lowenstein O, Loewenfeld IE. Pupillotonic Pseudotabes (Syndrome of Markus-Weill and Reys-Holmes-Adie): A Critical Review of the Literature. Surv Ophthalmol. 1965; 10: 129-185.
- Hardin WB Jr, Gay AJ. The phenomenon of benign areflexia. Review of the Holmes‐Adie syndrome with case reports and a study of the Achilles reflex. Neurology. 1965; 15: 613-621.
- Loewenfeld IE, Thompson HS. The tonic pupil: a re-evaluation. Am J Ophthalmol. 1967 Jan;63(1):46-87.
- Thompson HS. Adie’s syndrome: some new observations. Trans Am Ophthalmol Soc. 1977;75:587-626.
- Colak S, Erdogan MO, Senel A, Kibici O, Karaboga T, Afacan MA, Akdemir HU. A Rare Case in the Emergency Department: Holmes-Adie Syndrome. Turk J Emerg Med. 2016 Mar 2;15(1):40-2.
- Pearce JMS. The Myotonic (Holmes Adie) pupil. Adv Clin Neurosci Rehabil 2018;
- Xu SY, Song MM, Li L, Li CX. Adie’s Pupil: A Diagnostic Challenge for the Physician. Med Sci Monit. 2022 Mar 8;28:e934657.
- Sarao MS, Elnahry AG, Sharma S. Adie Syndrome. 2023 Jul 4. In: StatPearls
- Wakerley BR, Tan MH, Turner MR. Teaching video neuroimages: acute Adie syndrome. Neurology. 2012 Sep 11;79(11):e97.
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |