
![]()
An unusual wrist injury
aka Bone and Joint Bamboozler 008
A 30 year old man attends the Emergency Department after injuring his right wrist. He was playing rugby and landed awkwardly during a tackle with his hand trapped underneath another player. On arrival he is complaining of significant pain in his right wrist with reduced movement in all directions.
Examination:
- Examination of the wrist reveals reduced movement in flexion and extension and significant pain on pronation and supination.
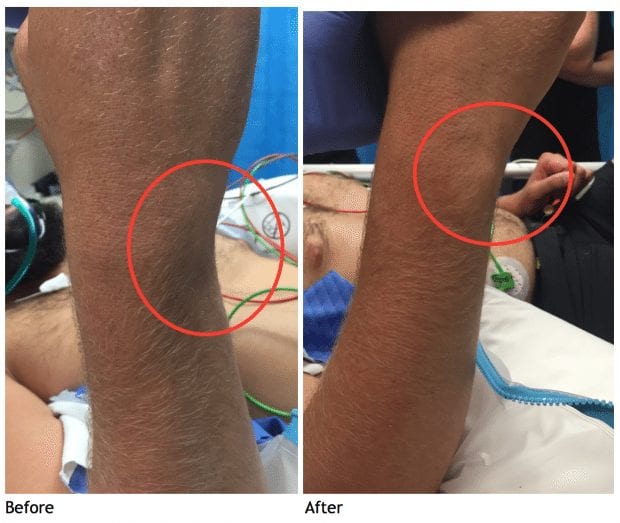
- You notice a hollow where his ulna styloid normally sits on the dorsum of his wrist.
Clinical Image of wrist on arrival

Investigation
A wrist XR is ordered…

Management:
- The patient is taken to Resus, where he is sedated with propofol and his wrist is manipulated.
- Before immobilisation you pause to review whether manipulation was successful.
Post manipulation clinical image
- His wrist is Cast immobilised in full pronation in a dorsal backslab.
- The post manipulation X-ray is shown below.
- The patient was discharged home with orthopaedic follow up arranged
Post manipulation XR

Clinical Questions, Interpretation and Explanation
What is the diagnosis?
Bamboozler Answer
Isolated volar distal radialulnar joint (DRUJ) dislocation
How are these injuries diagnosed?
Bamboozler Answer
History and Examination:
- The mechanism for isolated volar DRUJ dislocation is most commonly due to hyper- supination of the forearm, particularly with the hand in a fixed position.
- The patient presents with wrist pain, swelling and reduced ROM – particularly with pain on pronation.
- The tell-tale sign of a hollow where the prominent ulna styloid normally sits (as seen above) is not always obvious due to patient body habitus and swelling.
X-Ray:
- Postero-anterior (PA) view will show increased overlap of radius and ulna
- Lateral View demonstrates the distal ulna in a volar position
- Both these findings are seen on the x-ray in this case.
- A ‘true’ lateral is one in which the X-ray beam is centred between the two styloid processes (of ulna and radius) meaning the distal radius and ulna are superimposed on each other. Just a variation of 10 degree in either supination or pronation will result in an inaccurate lateral making assessing the DRUJ very difficult.
Other Investigations:
- Other investigations are required when the diagnosis is unclear or there are concerns of associated injuries which may alter initial management. These may include:
- CT scan is considered the best investigation for assessing DRUJ integrity and may demonstrate subtle subluxation or occult fractures both of which may not be visible on X-ray.
- MRI is useful for assessing associated ligamentous injuries.
- Arthroscopy is considered gold standard for assessing triangular fibro cartilage complex (TFCC) tears and allows repair if required.
How common are they?
Bamboozler Answer
Isolated DRUJ injury
- Isolated (i.e. with no associated fracture) DRUJ dislocation is very rare with dorsal dislocation thought to be more common than ulnar. It is a frequently missed diagnosis and as a consequence can lead to long term problems such as DRUJ instability and arthritis.
- DRUJ dislocation is often associated with injury to surrounding structures.
- The DRUJ stability is reliant on the integrity of the ulna and radius but also surrounding ligaments and muscles including triangular fibro cartilage complex (TFCC), ulna carpal ligament, extensor retinaculum, pronator quadratus and interosseous membrane.
Associated injuries to try to recognise in DRUJ dislocation include:
- Ulna styloid fractures
- Radial fractures
- Galeazzi Fracture – distal radial fracture with disruption of DRUJ.
- Essex-Lopresti Injuries – radial head fracture with interosseous membrane tear extending through DRUJ
Associated fractures make these injuries more unstable meaning they frequently require surgery. It is therefore prudent to involve your orthopaedic colleagues early if that is the case.
Note: There is also a high incidence of TFCC injury in DRUJ dislocations although the degree of damage is unclear. It is recognised that a complete DRUJ dislocation as in this case can cause only minor / incomplete TFCC injury and thus the decision to proceed with MRI or arthroscopy can be made at follow up in an orthopaedic outpatient clinic.
How is this injury best managed within the Emergency Department?
Bamboozler Answer
- Isolated Volar DRUJ dislocation can be reduced in the Emergency Department under sedation. This is done by applying dorsally directed firm pressure on the volar aspect of the distal ulna whilst forcibly pronating the forearm.
- The wrist is then cast immobilised in full pronation in a dorsal back-slab.
- A simple dislocation is diagnosed once post manipulation x-ray reveals normal alignment and no associated fractures. This patient can be followed up by the orthopaedic team in clinic (as occurred in this case).
- Complex dislocations that do not reduce or do not maintain normal alignment once reduced often need further imaging (CT is a reasonable starting point) and orthopaedic assessment in the ED.
References
- Stevens D. Distal Radioulnar Injury. LITFL
- Desault P-J. Extrait d’un memoire de M. Desault, sur la Luxation de l’extrémité inférieure du radius lu dans la Séance publique de l’Académie de chirurgie , en 1777, et non imprimé. Journal de Chirurgie 1791; 1(1): 78
- Schiller MG, af Ekenstam F, Kirsch PT. Volar dislocation of the distal radio-ulnar joint. A case report. J Bone Joint Surg Am. 1991 Apr;73(4):617-9.
- Kumar A, Iqbal MJ. Missed isolated volar dislocation of distal radio-ulnar joint: a case report. J Emerg Med. 1999 Sep-Oct;17(5):873-
- Mittal R, Kulkarni R, Subsposh SY, Giannoudis PV. Isolated volar dislocation of distal radioulnar joint: how easy to miss! Eur J Emerg Med. 2004 Apr;11(2):113-6.
- Thomas BP, Sreekanth R. Distal radioulnar joint injuries. Indian J Orthop. 2012 Sep;46(5):493-504.
- Werthel JD, Masmejean E, Silvera J, Boyer P, Schlur C. Acute isolated volar dislocation of the distal radio-ulnar joint: case report and literature review. Chir Main. 2014 Oct;33(5):364-9
- Bouri F, Fuad M, Elsayed Abdolenour A. Locked volar distal radioulnar joint dislocation. Int J Surg Case Rep. 2016;22:12-4.
CLINICAL CASES
Bone and Joint Bamboozler
Emergency Physician working in Western Australia. Areas of interest include ultrasound, sports injury and the eternal failures of Plymouth Argyle.
Had the exact same case a few months back. Key thing we found was that patient couldn’t supinate. Popped back in easy enough with sedation