![]()
Antibiotic Therapeutic Guidelines Update 2010
Therapeutic Guidelines is a valuable resource available in Australia for medical practitioners and healthcare professionals. It is an independant organisation which prepares guidelines using a panel of expert clinicians with the aim of distilling and interpreting the best available evidence and opinion at the time of publication. The information can be accessed via published hard copy books and in electronic form via the eTG.
The latest version of the New 2010 Antibiotic guidelines is an essential guide for the appropriate management of patients with infectious diseases in both general practice and hospital settings. All sections have been extensively reviewed and updated by a panel of experts, incorporating the latest evidence with a focus on clinical application. Major changes have occurred in the respiratory section; the recommendations for commonly used antibiotics and in the used of gentamicin therapy
Basic Drug Changes
- New drugs listed include doripenem, anidulafungin and micafungin
- Cefalotin (aka cephalothin) has been largely replaced by cephazolin. Cefalotin is now only recommended for directed therapy of serious staphylococcal infections sas the short half-life of cefalotin provides inadequate Gram-negative coverage.
- Safety issues regarding ceftriaxone and calcium-containing intravenous solutions are highlighted (e.g. reported deaths in neonates from ceftriaxone-calcuim salt precipitants in the lungs and kidneys).
Respiratory tract infections
- This chapter has probably had the biggest overhaul, simplifying recommendations and making them more relevent to practice.
- Two new systems for assessing severity of community-acquired pneumonia in adults (CORB, SMART-COP) have been introduced (see Appendix 2.4) to replace the complicated Pneumonia Severity Index (PSI) that was recommended in the last two versions of the guidelines.
- These differ from the PSI which predicted mortality (not really very useful) and gives us a much more valuable prediction tool in terms of which pateints are going to need intubation or vasopressor support.
- Treatment for community-acquired pneumonia (CAP) in adults is now divided into two groups
- Mild cases requiring outpatient care: amoxycillin OR doxycycline OR clarithromycin (NOTE: roxythromycin has gone)
- Moderate and severecases needing inpatient management
- Moderate: Benzylpenicillin IV then oral amoxycillin PLUS either doxyciline OR clarithromycin
- Severe: Azithromycin 500mg IV daily PLUS either Ceftriaxone OR benzylpenicillin + gentamicin OR cefotaxime
- For severely ill adults and children with CAP consider staphylococcal pneumonia. Treatment for non-MRSA and MRSA staphylococcal pneumonia with di/flucloxacillin PLUS vancomycin is recommended until the specific resistance pattern is known.
- For children aged 4 months to less than 5 years with non-severe CAP, treatment duration with oral amoxycillin has been reduced to 3 days
- Hospital-acquired pneumonia (HAP). When determining treatment, the need to consider local pathogens and the patient’s recent antibiotic exposure and culture results is stressed. NOTE: The presence of bacteria in sputum or endobronchial aspirate cultures does not itself justify a diagnosis of HAP, and usually represents colonisation only.
- For Legionella pneumonia, treatment options are now given for mild and severe cases
- Mild: Azithromycin OR doxycicline
- Severe: Azithromycin and (ciprofloxacin OR rifampicin)
- The influenza section has been expanded to include discussion of novel strains and the need to prioritise treatment for people at highest risk of complications. There is a new section on management of people with severe influenza. Excellent information on diagnosis, treatement, at risk groups, resistance to therapy and prophylaxis.
- Severe pharyngitis/tonsillitis: Corticosteroids have been added as an adjunct to antibiotics to provide symptomatic relief
- Acute epiglottitis (supraglottitis): Treatment regimen includes Ceftriaxone OR cefotaxime PLUS dexamethosone 0.15mg/kg (up to 10mg)
- Pertussis: Prophylaxis is only recommended for high-risk contacts
Antimicrobial hypersensitivity (allergy) NEW CHAPTER
- New chapter details the types of hypersensitivity reactions, provides a guide to the diagnosis of antimicrobial hypersensitivity and immune mediated hypersensitivity reactions to anitmicrobials.
- Includes a table outlining the management of patients reporting penicillin hypersensitivity.[PDF]
Bone and joint infections
- Gram-negative osteomyelitis (use cefotaxime or ceftriaxone)
- Osteomyelitis involving fracture fixation devices (pins, plates, screws) same principles apply as to arthroplasty devices
Cardiovascular system infections
- Streptococcal endocarditis is usually penicillin-sensitive, including Streptococcus bovis endocarditis
- Enterococcal endocarditis is intrinsically more resistant and should be treated with gentamicin plus penicillin
- Infected implantable cardiac devices (pacemakers, cardioverter-defibrillator infections) should be removed and empiric vancomycin + gentamicin administered until organism cultured
Central nervous system infections
- Cornerstone of diagnosis and treatment remains CSF based. However the guideline emphasises the importance of administering antimicrobials without delay once the clinical diagnosis is made and blood cultures have been taken
- Increased role of nucleic acid testing of the CSF in the diagnosis of meningitis is emphasised
- The need to consider clinical signs of raised intracranial pressure when determining the safety of a lumbar puncture is included in the algorithm for management of suspected bacterial meningitis in adults and children [PDF]
- The recommended dosing interval for vancomycin in meningitis has changed and is now 12-hourly
- New sections on eosinophilic meningitis, Streptococcus suis meningitis and recurrent benign lymphocytic meningitis
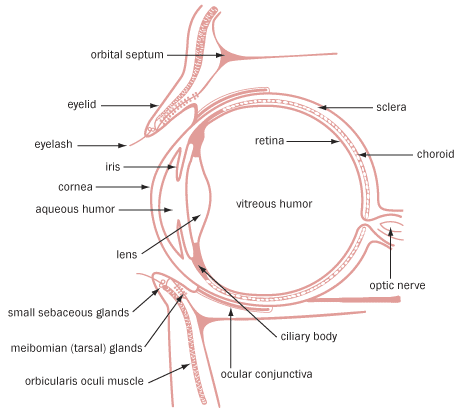
Eye infections
- A simple schematic diagram of the eye has been included to assist in understanding infections affecting different structures of the eye.
- Trachoma: (chronic Chlamydia trachomatis conjunctivitis) is the leading cause of preventable blindness in the world). Azithromycin is recommended for the management of all patients, including neonates.
{kind=link}
Genital and sexually transmitted infections
- New section on proctitis and more diagnostic information has been added
- Bacterial vaginosis: metronidazole vaginal gel is now recommended as an alternative option to the oral formulation
HIV infection
- Updated tables on antiretroviral drug dosages and adverse effects and prophylaxis and treatment of opportunistic infections in HIV-infected adults.
Intra-abdominal infections
- In the light of recent clinical trials antimicrobial prophylaxis is no longer recommended for severe necrotising pancreatitis or severe non-necrotising pancreatitis. Probiotic prophylaxis is also not recommended because of lack of benefit and possibility of harm
Malaria
- As usual there are multiple changes to this section
- The fifth human malaria parasite, Plasmodium knowlesi, is mentioned and treatment given
- Mild infections are treated as uncomplicated Plasmodium falciparum infection. Severe P. knowlesi infection is treated as for severe malaria.
- Mefloquine has been deleted as a treatment option for uncomplicated Plasmodium falciparum due to increasing resistance (especially in South-East Asia) and increased toxicity at treatment doses.
- Separate treatment recommendations are given for Plasmodium vivax depending on the region of acquisition and hence the likelihood of chloroquine resistance.
- Primaquine is now recommended concurrently with treatment of blood-stage infection to eradicate liver stages.
- The combination of proguanil plus chloroquine is no longer recommended for prophylaxis.
- Hydroxychloroquine is recommended as an alternative to chloroquine in adults where chloroquine is not available.
Mycobacterial infections
- An important discussion on drug-susceptible versus drug-resistant tuberculosis has been added.
- The dosing table for drugs used in tuberculosis has been revised and extended to include patients weighing 80 kg or more
- New section on the use of corticosteroids in TB. Corticosteroids should be used in the first few weeks of treatment of tuberculous pericarditis and meningitis and may speed resolution of tuberculous pleural effusions.
Modern antituberculosis regimens for fully susceptible organisms should have an initial cure rate of over 98% and a five-year relapse rate of less than 5%. Isoniazid resistance is found in 7% to 10% of Mycobacterium tuberculosis isolates in Australia, predominantly in patients born overseas and in those with a history of treated TB. Multidrug resistance (MDR) (resistance to at least isoniazid and rifampicin) remains uncommon in Australia (about 1% to 3% of isolates)
- The section on Mycobacterium ulcerans has been revised to reflect current Australian practice – rifampicin plus a quinolone for 8 weeks +/- conservative surgery
- For Mycobacterium avium complex, the need for macrolide susceptibility testing before commencing treatment is mentioned. A paragraph has been added about staged introduction of treatment to increase tolerance. Guidance is given on patients who are unsuitable for a three-times-weekly regimen
Urinary tract infections
- This chapter has been restructured into recommendations for adults and children as separate sections.
- In particular, due to difficultly in differentiating between cystitis and pyelonephritis in children, recommendations are given for mild (afebrile, no nausea or vomiting) or severe infection
- Nitrofurantoin is now recommended 12-hourly for acute cystitis in women and is no longer recommended in men. Nitrofurantoin is no longer recommended for prevention of infection in adults
- A doxycycline regimen is given for chronic prostatitis due to Ureaplasma or Chlamydia trachomatis.
Prophylactic Therapy
- Prevention of recurrent rheumatic fever: Phenoxymethylpenicillin is now only recommended for patients who refuse or cannot tolerate benzathine penicillin.
- Prevention of infection in joint prostheses: Prophylaxis is not recommended for patients with joint prostheses undergoing invasive procedures
- Prophylaxis for cirrhotic patients with GI bleed: Prophylaxis is now recommended regardless of whether patients are undergoing endoscopy
- Occupational post-exposure prophylaxis: New section on post-exposure prophylaxis against human T-cell lymphotropic virus type I (HTLV-I)
- Cardiovascular surgery: Duration of prophylaxis has been increased to 24 hours and the duration of prophylaxis for vascular surgery has beendecreased to 24 hours.
Other
- Severe Sepsis is now also referred to as sepsis syndrome.
- New section on community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) necrotising infection.
- Australian spotted fevers and scrub typhus: azithromycin recommended
- Q fever: Trimethoprim+sulfamethoxazole recommended in children 8 years or less and in pregnant women
- Typhoid and paratyphoid fevers: Azithromycin recommendation added for regions with decreased susceptibility to ciprofloxacin
- Varicella (chicken pox):The importance of treatment in pregnant women is emphasised.
- Pregnancy and Breastfeeding risk categorisations have been added for
- anidulafungin, aztreonam, daptomycin, darunavir, doripenem, ertapenem, etravirine, maraviroc, posaconazole, raltegravir, sulfadiazine, tigecycline, tipranavir.
Monitoring antimicrobial blood concentrations
Aminoglycosides
- Empirical therapy now recommended for a maximum of 48 hours (ie one, two or three doses depending on renal function). Caveat added to all empirical gentamicin recommendations that subsequent therapy should be guided by susceptibility results. Monitoring of blood concentrations is not required for this short-term empirical use.
- Directed therapy now limited to a few indications (infections when resistance to other safer antimicrobials has been shown, combination therapy for serious Pseudomonas aeruginosa infections and brucellosis, low doses as synergistic treatment for streptococcal and enterococcal endocarditis). Monitoring should commence on the first dose and the results should be used to guide subsequent doses.
- Graphical methods for monitoring blood concentrations (which had significant limitations) have been deleted.
Vancomycin
- For intermittent dosing, a higher starting dose is recommended in adults and children 12 years or more. Target trough concentration is now 15 ± 3 mg/L. Separate recommendations are given for infusion rates in adults and children.
- A section on continuous infusions has been added.
Renal impairment and antimicrobial dosing
- Recommendations have been added for the following medications
- abacavir+lamivudine, efavirenz+emtricitabine+tenofovir, atovaquone+proguanil, daptomycin, darunavir, doripenem, ertapenem, etravirine, maraviroc, nystatin, raltegravir, tigecycline and tipranavir.
The authors of the TG point out that the guidelines are not meant as a teaching tool, but rather to assist prescribers in ensuring patients receive optimum treatment. However, I believe these guidelines have developed into much more than a list of drugs and doses. There is extensive information on epidemiology, diagnosis and adjunctive treatments as well as drug therapy that can improve practice and ensure we do the best for our patients.
As you can see from the description of the changes above, there have been many updates and inclusion on the previous version of the Antibiotic Guidelines. Many uncommon microbial infections are discussed, but real usefulness is particularly seen in the central nervous system infection and respiratory infection chapters. Some of these updated evidence based recommendations will change the prescribing habits of the next generation of doctors.