
![]()
Auto-appendicectomy
Auto-appendicectomy (auto-appendectomy) is the surgical removal of one’s own appendix. The term sits within the broader realm of self-operation (auto-chirurgy) where a clinician performs a procedure on themselves, typically under local anaesthesia, out of necessity or a desire to demonstrate feasibility.
In appendicitis, self-operation is rare, but has been documented in three high-profile cases that span elective self-experimentation in a hospital, wartime isolation, and polar expedition medicine.
Self-appendicectomy is best understood as an intersection of anatomy, anaesthesia, and circumstance. Appendicectomy is “doable” under local infiltration, but the operator faces the constraints of limited exposure and orientation, fatigue, sterile field, and the practical requirement for assistants who can be directed to retract, light, and sometimes close.
Operations
February, 15 1921
Evan O’Neill Kane (1861-1932), country surgeon and railway accident specialist performed a self-appendicectomy under local anaesthesia in a hospital setting. Kane published the case to support “major” surgery under local infiltration.
Kane describes a history of chronic appendicitis, minimal prep (“one day’s starvation” and oil), walking to hospital, premedication with morphine, then announcing (to everyone’s alarm) that he would perform the operation himself. He positioned himself semi-sitting with the table head raised, pillows under his shoulders, a foot brace to flex hips/knees, and had the anaesthetist push his head forward so he could see the field.
- Incision planning: mapped the site “one inch below McBurney’s point,” planned a 3.5 inch diagonal incision (larger than he preferred in routine cases because he “did not know what to expect” in himself).
- Local anaesthesia: infiltrated locally with “cocain and adrenalin” (not novocaine as frequently quoted) into skin and deeper abdominal wall. Kane noted the striking the peritoneum produced a “sharp prick” sensation. He then waited ~4 minutes before incision.
- Finding the appendix: Kane reports no adhesions and lifting the caecum exposed the appendix. It appeared enlarged/injected with concretions. He then had an assistant hold it up under tension while he ligated in the usual way.
- Closure: Kane states he left wound closure to his assistants
August 1944
Robert Kerr “Jock” McLaren (1902–1956) (Mindanao / Borneo). Australian commando whose reported self-appendicectomy occurred while operating behind enemy lines. The story survives primarily through biographical accounts rather than a contemporary medical report.
Accounts describe McLaren becoming progressively unwell while moving between guerrilla positions and concluding he had appendicitis with no prospect of evacuation. He is variously described as having veterinary training and as taking charge of the operation when no surgeon was available. A makeshift set-up is described (improvised table, basic instruments), with no general anaesthetic and (in the best-known version) mirror guidance to visualise the wound.
Reported conduct of the operation: a right lower quadrant incision (with a razor) is described, with progressive opening of the abdominal wall (utilising blunt dissecvtion with two spoons…). Identification and removal of a ruptured appendix, followed by closure using improvised materials (including “jungle/banana fibre”). Duration is commonly given as several hours (often ~4–5 hours).
Historical caution: later reporting is inconsistent on key points (exact location, whether he performed the excision himself versus directing others, and the degree of assistance). Best presented as a remarkable reported self-operation with disputed procedural details, supported by later narrative sources rather than a primary surgical case report.
April 30, 1961
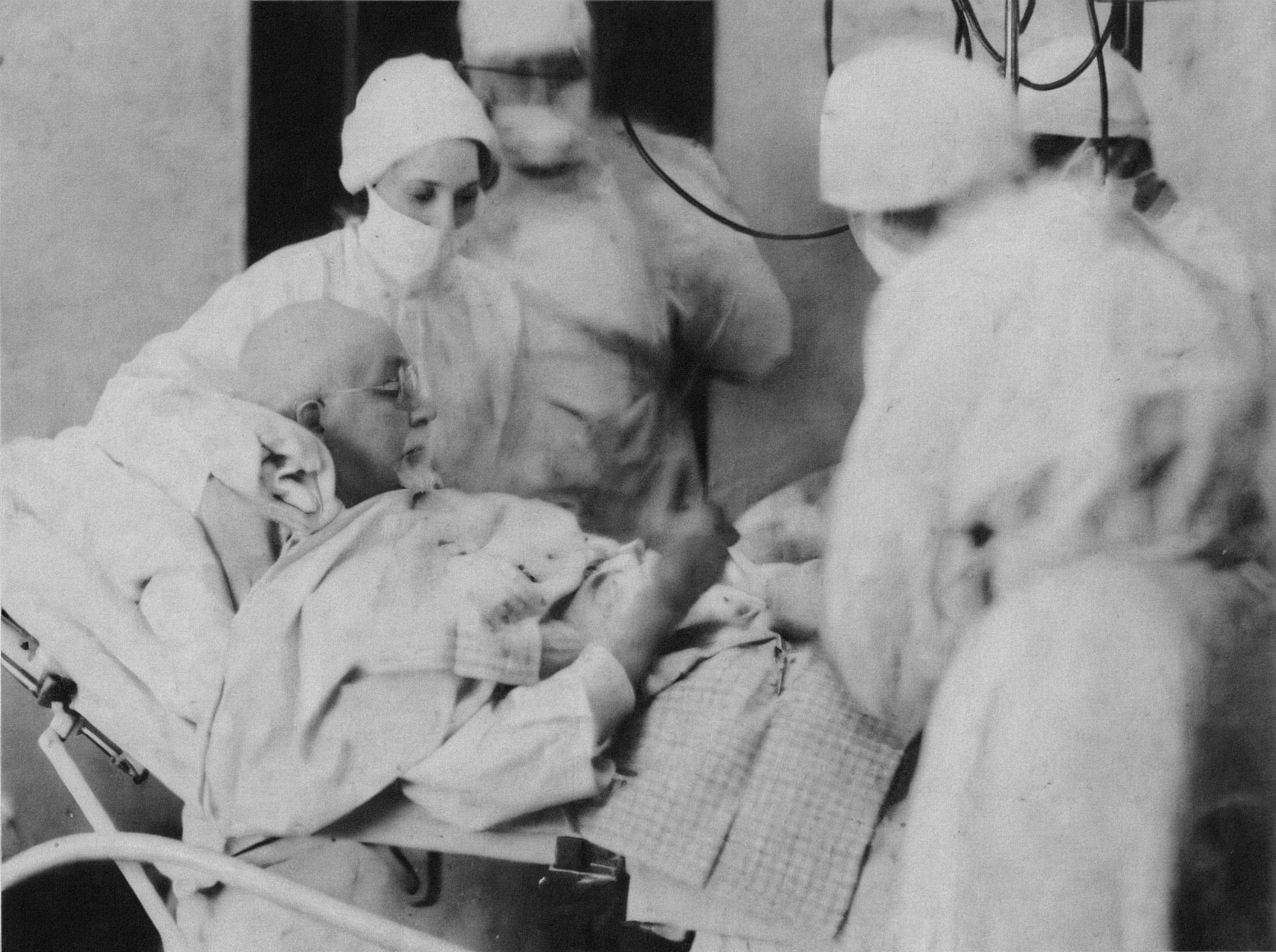
Leonid Ivanovich Rogozov (1934-2000). Sole doctor at Novolazarevskaya Station who performed a self-appendicectomy under local anaesthesia during a blizzard when evacuation was impossible. His 1962 first-person account was later published in English translation.
Operation (April 30, 1961, late evening)
- Positioning – Semi-reclining, half-turned to the left, weight on left hip; lower body elevated ~30°, minimising mirror use.
- 22:00 (Moscow time) – Abdominal wall infiltrated with 0.5% novocaine.
- 22:15 – “typical” incision of 10–12 cm
- Mirror use – Used for: exposing the peritoneum, suturing the peritoneum, and finding the appendix (steps requiring precision where the wound depth was hard to see). Otherwise he mostly operated without it, sometimes by feel.
- Intra-op physiology – After 30–40 minutes: marked weakness and vertigo → short rests required.
- Findings – Appendix “severely diseased” with a 2 × 2 cm perforation at its base.
- Completion – Antibiotics placed in the peritoneal cavity; wound closed; operation finished at midnight.

Associated Persons
- Evan O’Neill Kane (1864–1932) – 15 February 1921
- Robert Kerr “Jock” McLaren (1902–1956) – August 1944
- Leonid Ivanovich Rogozov (1934–2000) – 30 April 1961
References
- Pankratz L. Do It to Yourself Section: Surgery. JAMA. 1986;255(3):324.
- Nwaogbe C, Simonds EA, D’Antoni AV, Tubbs RS. Surgeons performing self-surgery: A review from around the world. Translational Research in Anatomy. 2018;10:1–3.
- Radhakrishnan J, Koo N. Atypical appendectomies. Hektoen International. 2021.
Kane operation
- Kane EO. Autoappendectomy (a case history). International Journal of Surgery. 1921;34(3):100–102.
- Rennie D. Do It to Yourself Section: The Kane Surgery. JAMA. 1987;257(6):825–826.
Rogozov operation
- Rogozov LI. Self Operation. Soviet Antarctic Expedition Information Bulletin. 1964;4:223–224.
- Rogozov V. Operace vlastního apendixu v Antarktidě. Práce jako práce, život jako život. Vesmír. 2004;83(1):25.
- Rogozov V, Bermel N. Auto-appendectomy in the Antarctic: case report. BMJ. 2009;339:b4965.
- That self-appendectomy. Amundsen-Scott South Pole Station.
McLaren operation
- Richardson H. One-man War: The Jock McLaren Story. Adelaide: Griffin Press; 1957.
- Gilling T. Bastard Behind the Lines: The Extraordinary Story of Jock McLaren’s Escape from Sandakan and His Guerrilla War Against the Japanese. 2021.
eponymythology
the myths behind the names

DM (UWA), BM (Indiana), FMusA, LMusA. Resident Medical Officer, Sir Charles Gairdner Hospital. Basic Surgical Streaming Program. Professional violinist, now aspiring surgeon. Loves music, opera, and operating.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |