
![]()
Broken-hearted chest drain
aka Cardiovascular Curveball 001
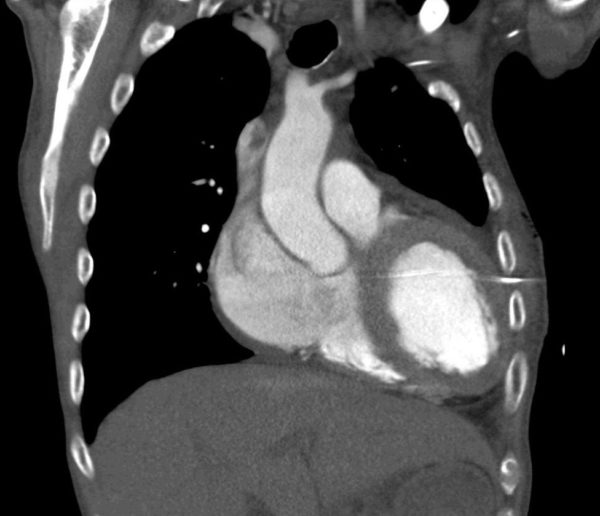
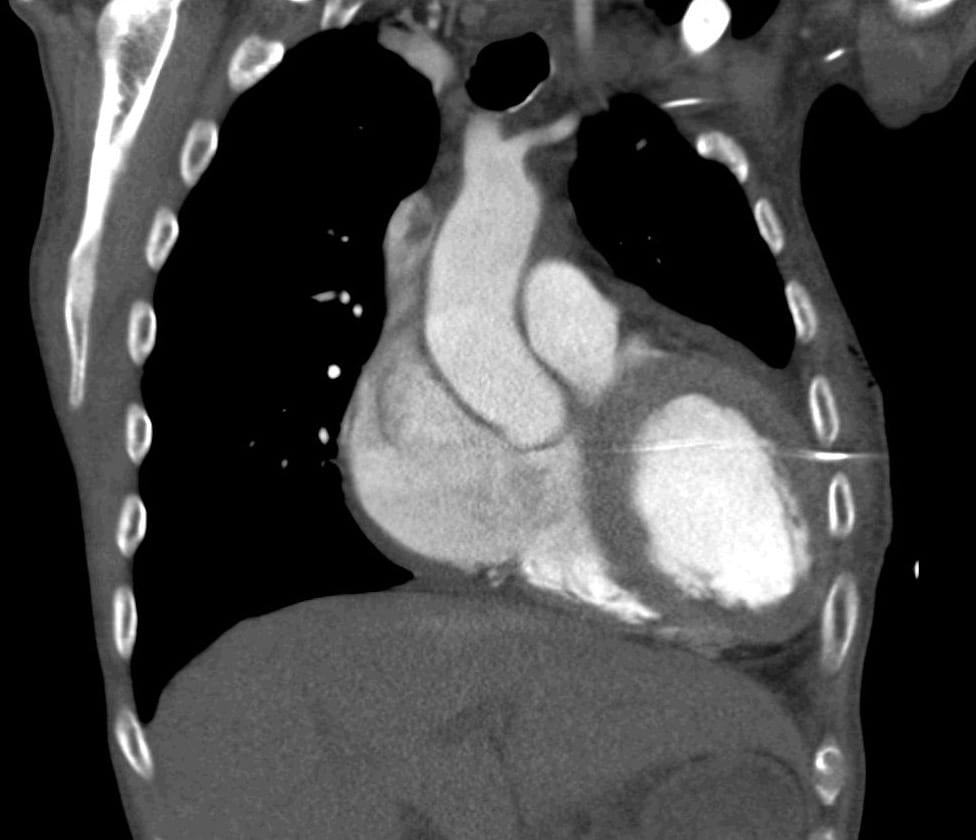
An 86 year-old male presented with shortness of breath.He developed a complication after insertion of a left chest drain. Here is his CT:

Q1. What is the complication?
Curveball Answer
The chest drain is in the left ventricle.
Q2. Outline your management.
Curveball Answer
This complication was identified at the time by the presence of pulsatile bright red blood coming from the drain.
- Clamping the drain to prevent exsanguination is a good first step!
- Not taking the drain out is a good second step.
- The next step is to prepare the patient for cardiac surgery to remove the drain and repair the heart. In this patient, removing the drain and repairing the heart was achieved via a mini thoracotomy.
In addition to the issues of patient care, this is a sentinel event and appropriate reporting and follow-up needs to be undertaken. The CT below demonstrates how this complication arose…not everything that looks like a left pleural effusion on a plain chest X-ray is one!
{kind=link}
Q3. How could this complication have been prevented?
Curveball Answer
Put your finger in the hole!
One of the most important steps in the insertion of an intercostal catheter is to insert a finger through the hole you have just made. Do this before inserting the intercostal catheter.
Using your finger you can detect any adhesions that may lead to penetration of the lung on insertion of the intercostal catheter, as well as the presence of underlying organs such as a beating heart!
In this case, the intercostal catheter is a one from a Seldinger kit. If you are going to use one of these kits, you should do an ultrasound to make sure that there really is a pleural effusion that can be safely drained.

CLINICAL CASES
Cardiovascular Curveball
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC

Great post Chris. I have seen this complication as well. Another teaching point is on the left, seldinger chest tubes should be landmarked at the mid or posterior axillary line (and confirmed with US). In contrast to the right chest, the the anterior clavicular line abuts the LV. Also – do not use the trochars that come with most kits. Finally, if you do adynamic US and mark the money spot, do not reposition the patient or their bed angle afterwards – small changes in position can cause big changes to anatomy.