![]()
Alpha-Gal Syndrome
Alpha-gal syndrome explained: tick bites, delayed red meat allergy, cetuximab anaphylaxis, and the clues that linked them.

![]()
Alpha-gal syndrome explained: tick bites, delayed red meat allergy, cetuximab anaphylaxis, and the clues that linked them.
Fluorescein: history, chemistry and modern eye uses—corneal staining, Seidel leak test, Jones drainage test and retinal angiography.
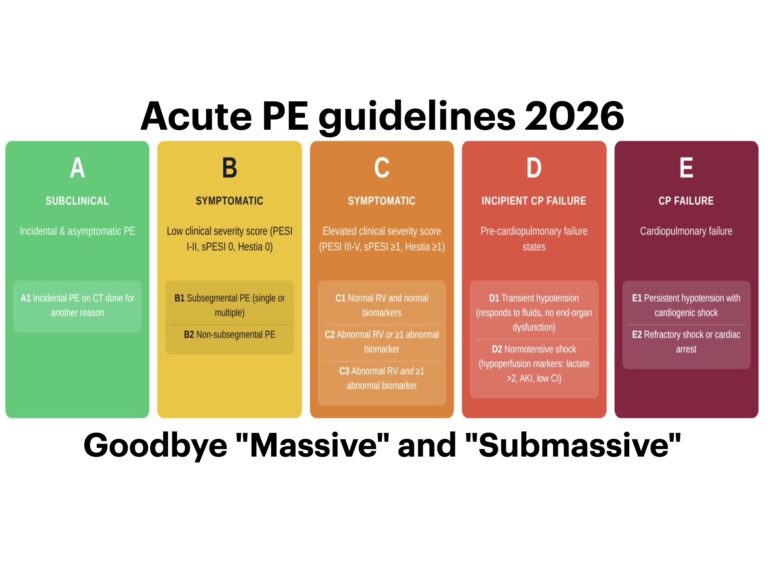
The first-ever AHA/ACC clinical practice guideline on acute pulmonary embolism drops a new A-to-E severity classification. Here’s what emergency physicians need to know...
George Philo Pitkin (1885-1943), American surgeon. Inventor of Spinocain, Pitkin spinal needle, syringe and tiltometer for controllable spinal anaesthesia.

A 45 year old female presents with shoulder pain following a seizure. Describe and interpret the CT scan of her left shoulder
John Snow (1813-1858), English physician. Pioneer of anaesthesia and epidemiology. Defined etherization stages and traced cholera outbreaks to contaminated water in London.
Emery A. Rovenstine (1895–1960), American anaesthesiologist linked to directional spinal needle, nerve block and geriatric anaesthesia.
Charles Gabriel Pravaz (1791–1853). French orthopaedic surgeon developed the Pravaz syringe, an early controlled injection device for aneurysm treatment.
Josef Thurner (1927-2025), Austrian pathologist; May–Thurner syndrome; led pathology in Salzburg; published widely on venous disease.
Gaston Labat (1876–1934). Regional anaesthesia pioneer, author of Regional Anesthesia, founder of ASRA, and namesake of the Labat sciatic block, Labat spinal needle and Labat outfit
Lincoln Fleetford Sise (1874-1942). Lahey Clinic anaesthetist known for fine-gauge spinal needle introducers and safer spinal anaesthesia.
Barnett Alan Greene (1907-1999) American anaesthesiologist. Use of fine-gauge obstetric spinal needles and reducing post-spinal headache.