
![]()
Central Pontine Myelinolysis
Central pontine myelinolysis (CPM), also known as osmotic myelinolysis, is a rare condition that may result in death or severe, largely irreversible neurological disability.
CPM is usually seen as an iatrogenic condition resulting from excessively rapid correction of chronic (>48 hours) hyponatraemia with saline solutions.
Although there is no universally agreed rate of correction, most experts suggest that serum sodium should not rise by more than 10–14 mmol/L over 24 hours.
History
Central pontine myelinolysis was first described by Raymond D. Adams et al in 1958 in patients with a background of alcoholism and malnutrition. The characteristic histopathological finding was a symmetrical central zone of myelin destruction in the pons with sparing of axons and nerve cells. Quadriplegia and pseudobulbar palsies were the main clinical findings.
B. E. Tomlinson et al published case reports of two patients presenting with hyponatraemia in 1976. They were and treated with rapid sodium correction resulting in rapid alteration in consciousness and the development of quadriparesis and dysphagia. There was no history of alcoholism or malnutrition.
Pathology
Nature of the Condition
CPM is a demyelinating condition, the exact pathology of which remains unknown, but may relate to sudden osmotic changes affecting neurons.
There are no inflammatory or vasculitic changes.
Sites of Involvement
- Predominantly affects the central portion of the pons.
- Extra-pontine myelinolysis (EPM) occurs in ~10% of cases, involving other areas of the CNS.
Causes
1. Rapid Correction of Chronic Hyponatraemia
- Most common cause.
- Occurs when correction exceeds the brain’s ability to adapt to a higher osmolality.
- Note: Many patients (~75%) who have their sodium corrected too rapidly do not develop CPM, suggesting other unrecognised risk factors may exist.
2. Chronic Alcoholism and Malnutrition
- Originally described in chronic alcoholics and malnourished patients.
Risk Factors
Principal risk factors in iatrogenic cases include:
- Serum sodium levels:
- Initial serum sodium < 120 mmol/L (rare above this).
- Hyponatraemia present for >48 hours.
- Chronic alcoholism.
- Malnourishment.
- Hypokalaemia.
- Elderly patients on long-term thiazide diuretics.
Clinical Features
Symptom Onset
Symptoms typically develop progressively over 3–5 days after excessively rapid correction of hyponatraemia.
Clinical Presentation
- Confusion.
- Altered conscious state.
- Seizures.
- Brainstem signs, including:
- Nystagmus.
- Ocular motor lesions (esp. sixth nerve palsy).
- Dysarthria / pseudobulbar palsy.
- Dysphagia.
- Quadriparesis.
- Brainstem lesions are usually symmetric.
- Extensive lesions may cause locked-in syndrome (paralysis of lower cranial nerves and limb muscles).
- Some incomplete improvement may occur over weeks to months, but permanent deficits are common.
- Cases of complete recovery have been reported.
Differential Diagnoses
Consider:
- Brainstem stroke.
- Multiple sclerosis.
- Brainstem tumours (gliomas).
Investigations
Diagnosis
- Diagnosis is based on clinical findings and MRI scan.
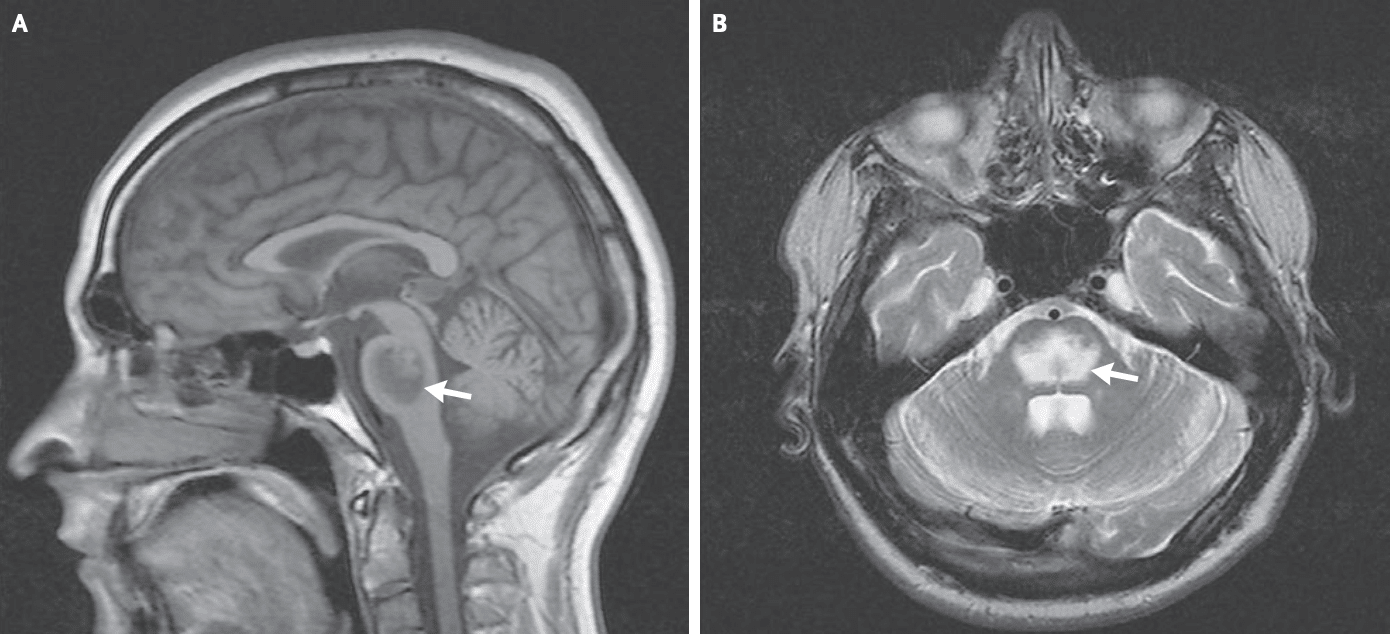
A. Well-defined lesion in the pons of low T1-signal intensity. B. High T2-signal intensity (Fleming, 2008)
Management
- No specific treatment exists for CPM.
- Management is entirely supportive.
- If rapid correction is recognised, lowering serum sodium (e.g. with desmopressin) may be attempted to mitigate risk.
References
Publications
- Adams RD, Victor M, Mancall EL. Central pontine myelinolysis: a hitherto undescribed disease occurring in alcoholic and malnourished patients. AMA Arch Neurol Psychiatry. 1959;81(2):154-72.
- Tomlinson BE, Pierides AM, Bradley WG. Central pontine myelinolysis. Two cases with associated electrolyte disturbance. Q J Med. 1976 Jul;45(179):373-86.
- Laureno R, Karp BI. Myelinolysis after correction of hyponatremia. Ann Intern Med. 1997 Jan 1;126(1):57-62.
- Pirzada NA, Ali II. Central pontine myelinolysis. Mayo Clin Proc. 2001 May;76(5):559-62.
- Fleming JD, Babu S. Images in clinical medicine. Central pontine myelinolysis. N Engl J Med. 2008 Dec 4;359(23):e29
- Danyalian A, Heller D. Central Pontine Myelinolysis. StatPearls, Aug 2023.
FOAMed
- Nickson C. Central Pontine Myelinolysis. CCC
- Nickson C. Hyponatraemia. LITFL
- Cadogan M. Hyponatraemia. CCC
- Farkas J. Hyponatremia. EMCRIT
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |