
![]()
Carpal Tunnel Syndrome signs
Carpal tunnel syndrome (CTS) is synonymous with multiple eponymous and semi-eponymous clinical signs. The best known are the Hoffmann–Tinel sign and Phalen test, both intended to reproduce paraesthesia in the median nerve distribution. Later tests, including Gilliatt–Wilson’s pneumatic tourniquet test, Durkan’s carpal compression test, and the pressure provocative test, demonstrate mechanical or ischaemic provocation of median nerve symptoms.
Modern diagnosis has moved away from isolated bedside signs toward pattern recognition. Individual tests vary by technique, force, duration, reference standard, and disease severity and none should be used alone. Symptom localisation tools include the Katz–Stirrat hand diagram and Boston / Levine questionnaire. Prediction rules such as the Wainner clinical prediction rule and CTS-6 combine symptoms, examination findings, and severity markers.
History of signs and tests in carpal tunnel syndrome
Carpal tunnel syndrome as a clinical entity
1854 – Sir James Paget (1814–1899) described two cases of median nerve compression at the wrist. The first followed constriction at the wrist by a tight cord and the second followed fracture of the distal radius with excessive new bone formation and compression of the median nerve. Paget did not define carpal tunnel syndrome but recognised the pathological effect of pressure on the median nerve at the wrist, and the clinical improvement when that pressure was relieved.
1880 – James Jackson Putnam (1846–1918) described recurrent nocturnal and early-morning paraesthesia, pain, numbness, and weakness of the hands (Putnam’s Acroparesthesia). Many patients described with acroparesthesia would now likely be recognised as having idiopathic carpal tunnel syndrome.
1911–1914 – James Ramsay Hunt (1872–1937) described thenar and hypothenar neural atrophy, emphasising wasting of the small hand muscles. He attributed thenar wasting to compression or neuritis of the median thenar branch near the anterior annular ligament and separated this motor syndrome from the sensory acroparesthesia tradition.
1912–1913 – Pierre Marie (1853–1940) and Charles Foix (1882–1927) analysed isolated non-progressive atrophy of the small hand muscles. They reported a case of isolated thenar atrophy due to median nerve pathology at the anterior annular ligament of the carpus. They suggested that early division of the anterior annular ligament could prevent progression.
1947 – W. Russell Brain (1895–1966), A. Dickson Wright, and Marcia Wilkinson demonstrated that spontaneous median nerve compression in the carpal tunnel could produce both median-distribution sensory symptoms and partial thenar atrophy. They reported six surgically treated cases in which division of the transverse carpal ligament produced rapid relief of pain and tingling.
1950–1966 – George S. Phalen (1911–1998) popularised the modern clinical understanding of carpal tunnel syndrome through large clinical series. He clarified the anatomy, diagnosis, and treatment by corticosteroid injection or carpal tunnel release. His publications made CTS widely recognisable in clinical practice.
Provocative signs in carpal tunnel syndrome
Provocative signs attempt to reproduce median nerve symptoms by percussion over the nerve, sustained wrist flexion, wrist extension, or direct carpal tunnel compression. Diagnostic performance varies as technique, force, duration, reference standard, and disease severity differ across studies.
1915 – Paul Hoffmann (1884–1962) and Jules Tinel (1879–1952) independently described mechanically induced distal tingling in injured peripheral nerves during the First World War. Hoffmann emphasised light percussion over a regenerating nerve whilst Tinel described pressure over an injured nerve trunk producing distal formication. In CTS, the Hoffmann-Tinel sign is used to test median nerve compression. It is positive when light tapping or percussion over the median nerve at the wrist reproduces radiating paraesthesia in the median nerve distribution.
1948 – George S. Phalen (1911–1998) introduced the wrist-flexion test in the late 1940s. The Phalen test asks the patient to allow both wrists to fall into complete flexion, for 30–60 seconds. Reproduction or worsening of median-distribution numbness or paraesthesia is positive. The commonly illustrated dorsum-to-dorsum version is a later modified Phalen variant, not Phalen’s original description.
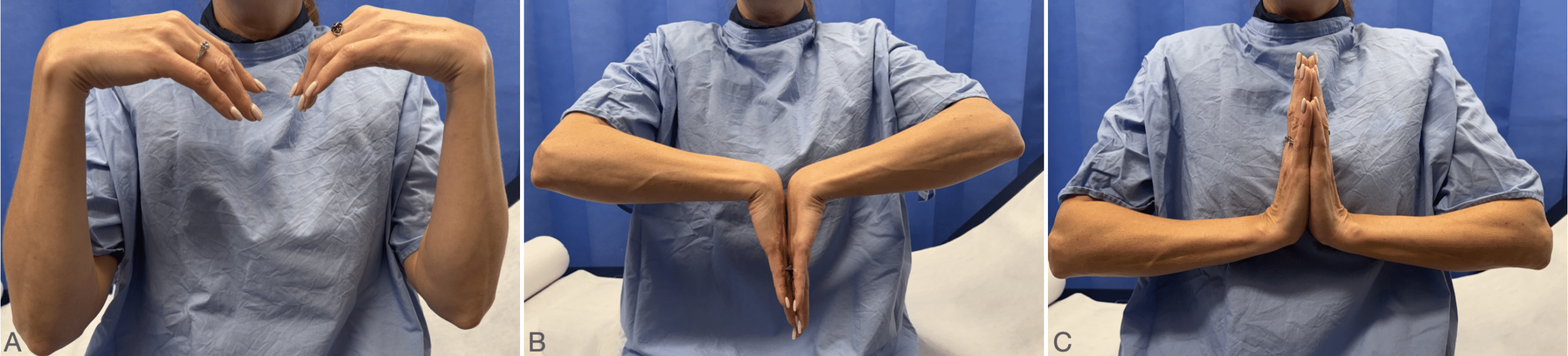
A. Classic Phalen wrist-flexion test: forearms vertical, wrists allowed to fall freely into flexion, hands not touching.
B. Modified Phalen test: dorsal surfaces of the hands placed together to maintain bilateral wrist flexion.
C. Reverse Phalen / Wormser test: palms together with wrists extended.
1950 – Peter Wormser discussed wrist dorsiflexion as a provocative factor in CTS. Later, the reverse Phalen manoeuvre was formalised as sustained wrist and finger extension, with the palms together in a “prayer” position. The test provokes symptoms by wrist extension rather than flexion. Experimental pressure studies suggest wrist extension can increase carpal tunnel pressure substantially, but diagnostic performance remains modest.
1953 – Roger W. Gilliatt and T. Grahame Wilson described a pneumatic-tourniquet test for CTS. A cuff was inflated around the arm above the elbow to arrest circulation. In affected patients, intense paraesthesia or early sensory loss appeared preferentially in the median nerve distribution. They found altered ischaemic paraesthesia in 13/35 suspected cases, especially in patients with frequent severe nocturnal symptoms. The test supported the concept that acroparaesthesia could result from median nerve compression at the carpal tunnel, but it is now mainly of historical interest.
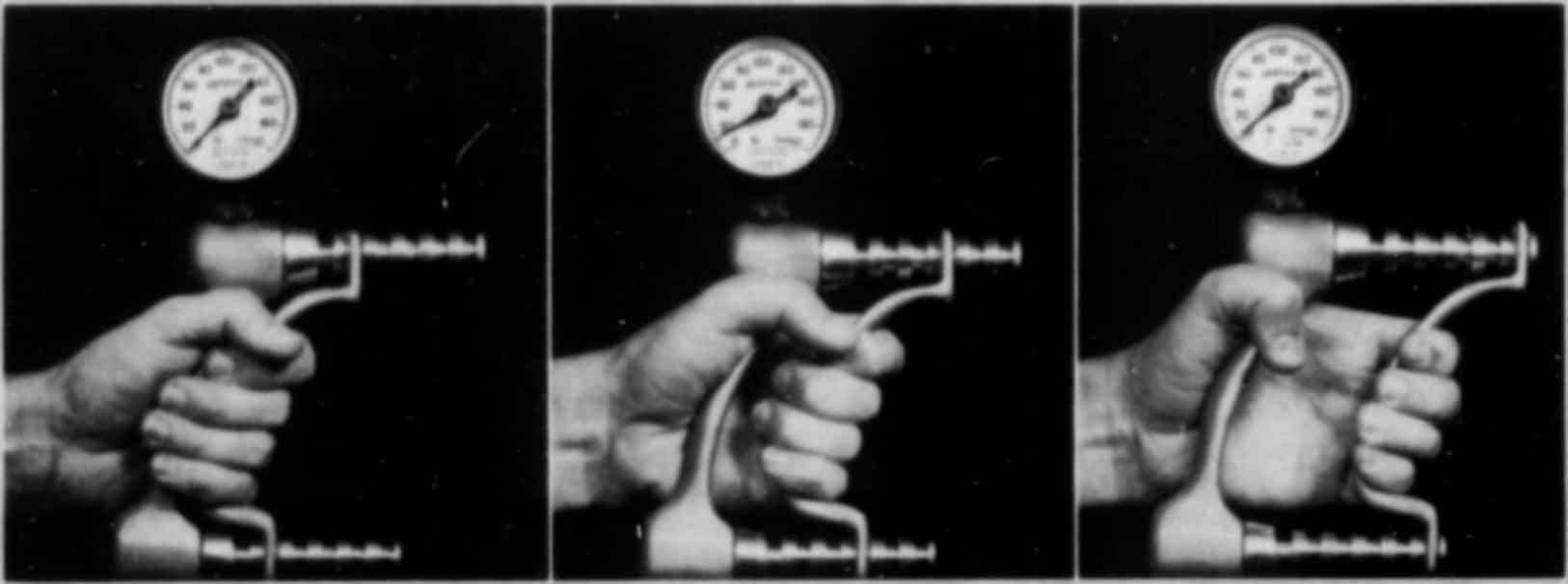
1991 – John A. Durkan introduced the carpal compression test, applying direct pressure over the carpal tunnel and underlying median nerve for up to 30 seconds. A positive test reproduces numbness, pain, or paraesthesia in the distal median nerve distribution. Durkan reported higher sensitivity and specificity than Phalen and Tinel in his original study. In 1994, Durkan introduced the Durkan CTS gauge to standardise the pressure applied during testing.

Right: Durkan pressure gauge. Durkan 1994
1992 – Tara M. Williams et al verified the pressure provocative test as a direct median nerve compression manoeuvre. Direct thumb pressure was applied over the median nerve at the wrist while a sphygmomanometer was used to standardise pressure at 100 or 150 mmHg. In their study of 30 CTS patients and 30 controls, the high-pressure test had sensitivity 100%, specificity 97%, and a mean symptom onset time of 9 seconds, faster than Phalen’s test at 30 seconds.
Symptom localisation and history tools
These tools document where symptoms occur, how patients relieve them, and how CTS affects daily function.

1984 – William E.M. Pryse-Phillips described and validated the flick sign as a history feature in carpal tunnel syndrome. The sign is positive when the patient reports or demonstrates shaking or flicking the hand to relieve nocturnal or activity-related paraesthesia. Pryse-Phillips reported that the flick sign predicted electrodiagnostic abnormality in 93% of cases, with a false-positive rate < 5%. Later studies did not reproduce such strong performance consistently. Sign is best treated as a useful history clue rather than a definitive diagnostic sign.
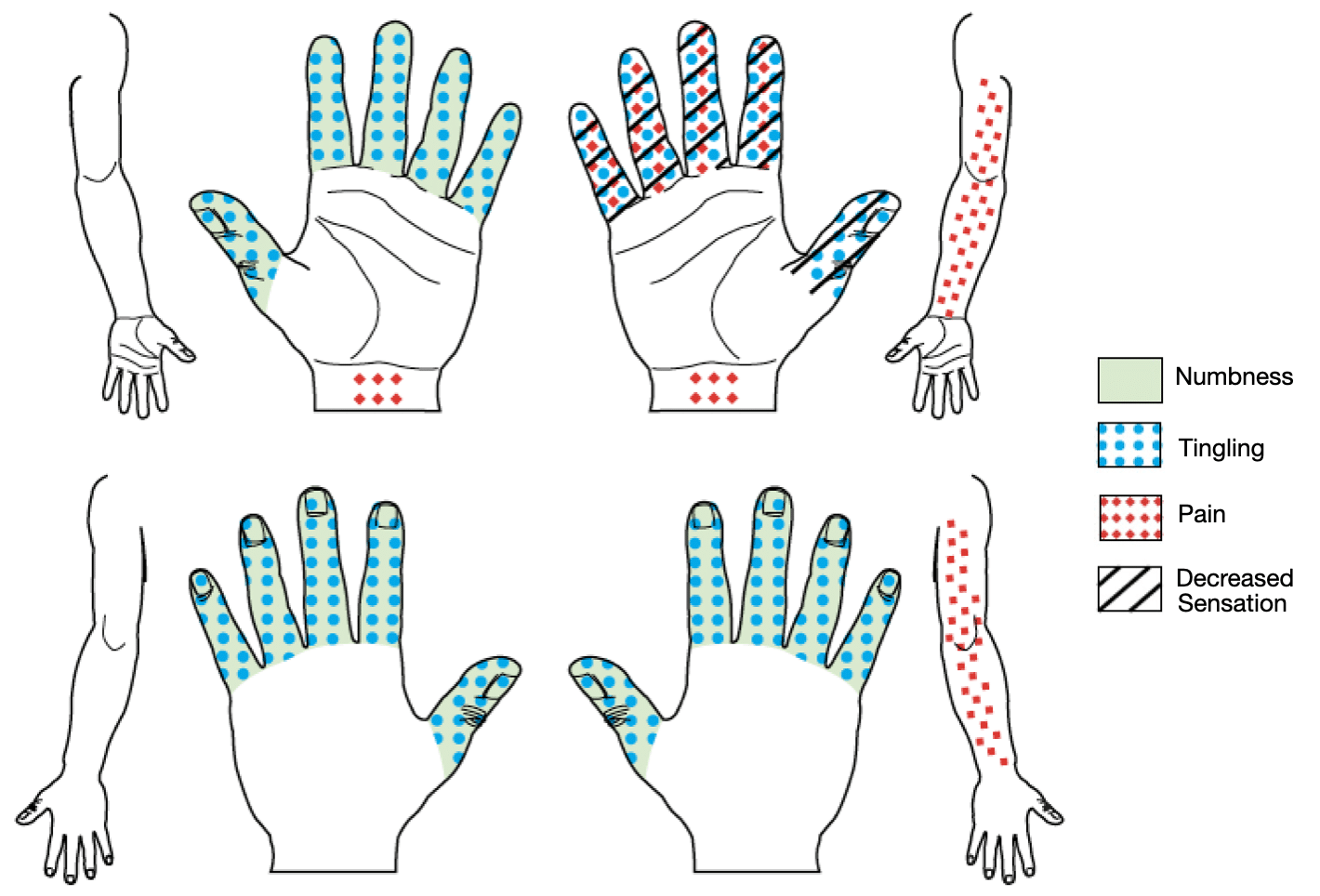
1990 – Jeffrey N. Katz and Craig R. Stirrat developed the self-administered Katz–Stirrat hand diagram to improve symptom localisation in patients with upper-limb paraesthesia. Patients mark the distribution of pain, numbness, tingling, or altered sensation on palmar and dorsal hand diagrams. The patterns are classified as classic, probable, possible, or unlikely CTS. Katz reported that a classic or probable diagram had sensitivity 0.64, specificity 0.73, and positive predictive value 0.58 against nerve conduction diagnosis.
1993 – David W. Levine et al developed a self-administered questionnaire to assess symptom severity and functional status in CTS. The Boston Carpal Tunnel Questionnaire (BCTQ) or Levine questionnaire, has two main components, a Symptom Severity Scale and Functional Status Scale. The patient-reported severity and outcome measure is often used in CTS research, treatment trials, and postoperative follow-up.
Sensory and motor assessment
Sensory and motor tests document impairment rather than provoke symptoms. They are most useful for severity grading, treatment planning, and recovery tracking.
1952 / 1960 – Josephine Semmes (1916–1998) and Sidney Weinstein (1922–2010) developed calibrated nylon monofilaments to quantify cutaneous pressure thresholds, The Semmes–Weinstein monofilament examination was used to study somatosensory loss after penetrating brain injury. The method later became widely used in peripheral nerve assessment, including Hansen disease, diabetic neuropathy, and entrapment neuropathies. In CTS, Semmes–Weinstein testing documents altered sensory threshold in the median nerve distribution, but it is not a diagnostic sign. In 1993 Weinstein introduced the Weinstein Enhanced Sensory Test (WEST) aimed at improving standardisation, calibration, and clinical usability.
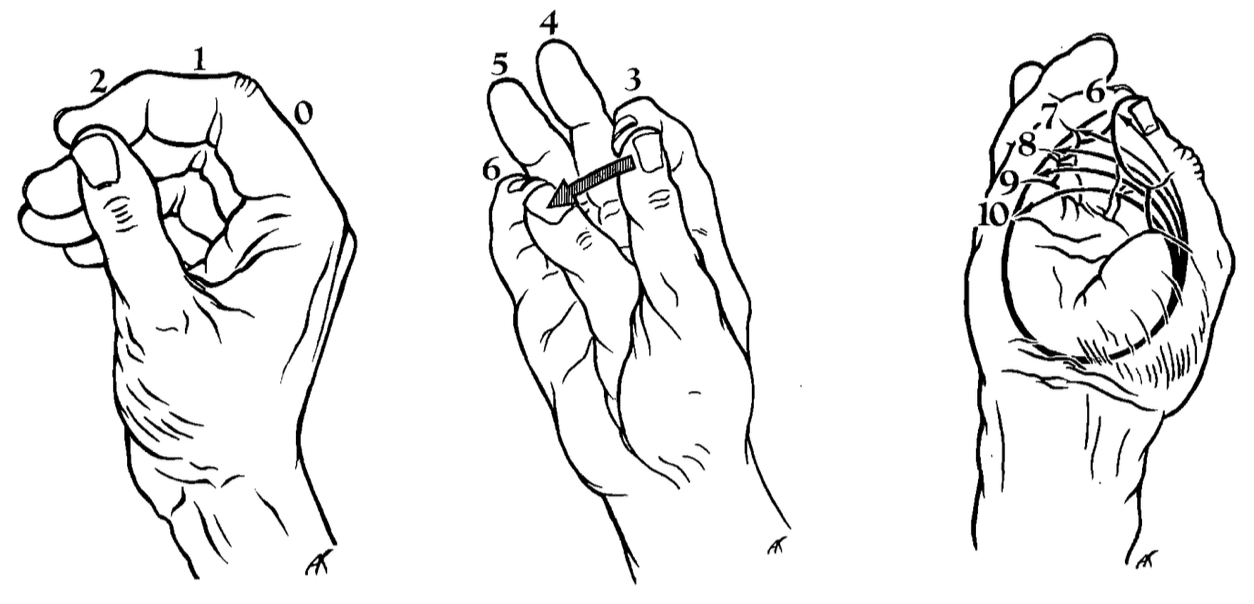
1986 – Adalbert Ibrahim Kapandji (1928-2019) described a clinical test of thumb apposition and opposition. The Kapandji opposition score grades true thumb opposition from 1–10, following the thumb tip from the radial side of the index finger, across the finger pulps, along the little finger, and finally to the distal palmar crease. In CTS the score is relevant as a functional assessment of thenar motor impairment and postoperative recovery. However it is not specific for CTS and should not be treated as a diagnostic test.
Static two-point discrimination tests the minimum distance at which two points applied to the fingertip are perceived as separate. In CTS it is used to document sensory impairment, especially in more advanced median nerve dysfunction. However, it is relatively insensitive for early CTS and technique-dependent. Buch-Jaeger used >6 mm at the index pulp as abnormal in their CTS clinical-sign study, but found low sensitivity.
Vibration testing ranges from bedside tuning-fork comparison to quantitative vibrometry. In CTS it assesses large-fibre sensory dysfunction and can document impaired median nerve function. Szabo et al. evaluated vibrometry, 256-Hz vibration, Semmes–Weinstein monofilaments, and two-point discrimination in CTS and distinguished threshold tests from innervation-density testing. Recent work using multi-frequency vibrometry found increased vibration perception thresholds across multiple frequencies in CTS patients compared with controls.
Thumb abduction strength testing. Weakness of thumb abduction reflects dysfunction of the abductor pollicis brevis, supplied by the recurrent motor branch of the median nerve. It is more likely in moderate to severe or longstanding CTS than in early disease. D’Arcy and McGee found thumb abduction strength testing more useful than many traditional provocative signs in distinguishing electrodiagnostically confirmed CTS, although normal strength does not exclude CTS.
Functional outcome measures
Functional outcome measures assess how CTS affects hand performance and impacts on daily life. These measures are useful for recording baseline severity, treatment response, and postoperative follow-up, not as stand-alone diagnostic tests.
1954 – Charles O. Bechtol described grip testing with a dynamometer with adjustable handle spacing, providing a reproducible way to quantify hand grip strength. He developed the JAMAR hydraulic dynamometer with the assiatnce of physical therapist Hyman Jampol (JAM), professor of engineering Morris Asimow (A), and prosthetics machinist Robert Reiss (R). In CTS, grip strength is useful for documenting functional impairment and recovery after treatment, but is not a diagnostic test for CTS.
1958 – Erik Moberg (1905–1993) published the Moberg pick-up test to assess functional sensibility by timing how quickly a patient picks up small objects, with vision and then without vision. Patients with CTS and median nerve sensory loss may suffer impaired tactile gnosis, object manipulation, and fine hand function.
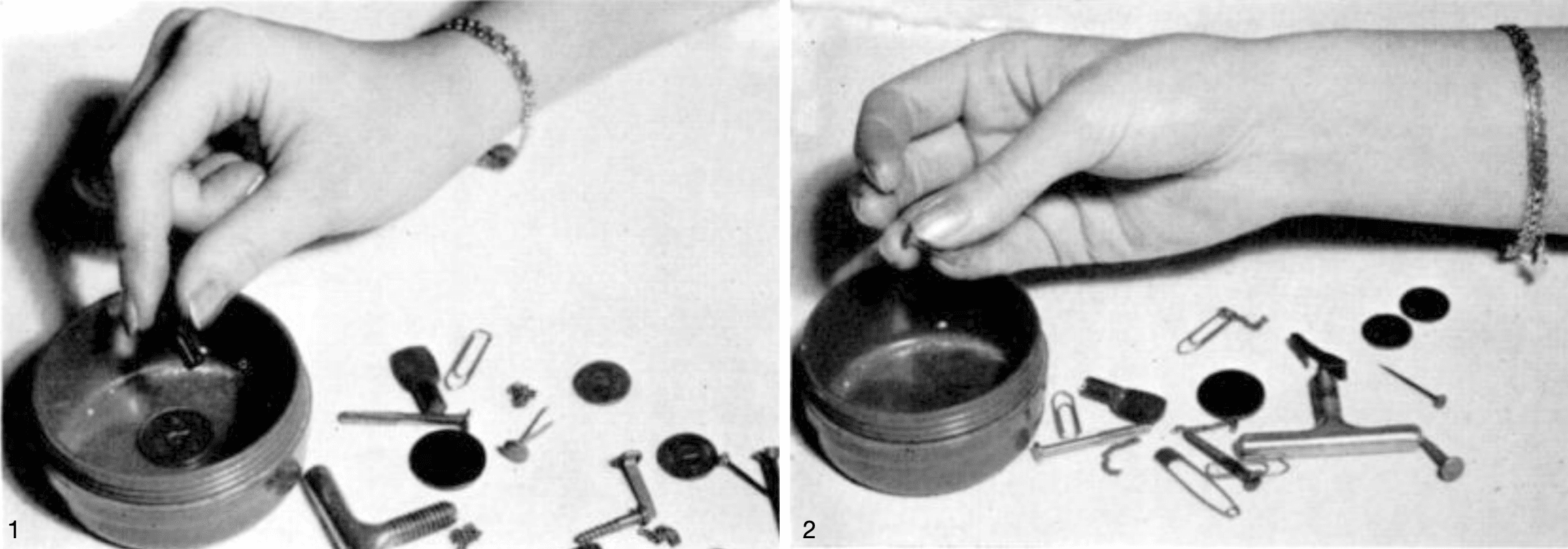
Figure 2: If sensibility in the median nerve region is impaired, the subject grasps an object with the thumb, together with the ring and little fingers. If the median nerve lacks tactile gnosis it cannot localise or identify objects. This area is “blind” Moberg pick-up test 1958
Prediction rules / modern synthesis
Prediction rules combine key symptoms and physical findings into a weighted score. They recognise that CTS is best diagnosed by a pattern of findings, not by a single positive Tinel, Phalen, or compression test.
1994 – Patrick Radecki described the square wrist ratio index as an anthropometric risk marker for CTS. A wrist ratio ≥0.7 was associated with median nerve abnormality in 79% of women and 87% of men in Radecki’s cohort. Included in Wainner’s clinical prediction rule.
2005 – Robert S. Wainner and colleagues developed the Wainner clinical prediction rule, a five-item clinical prediction rule for CTS. The five items include shaking the hand for symptom relief, square wrist ratio index >0.67, Symptom Severity Scale score >1.9, reduced median sensory field of the thumb, and age >45 years. With all five items positive, the likelihood ratio was 18.3 and when four were positive, the likelihood ratio was 4.6.
2008 – Brent Graham and colleagues developed the CTS-6, weighted clinical diagnostic criteria for CTS. The six clinical features include numbness predominantly in the median nerve distribution, nocturnal numbness, thenar weakness or atrophy, positive Phalen test, positive Tinel sign, and loss of two-point discrimination. It gives a weighted score rather than relying on any one sign alone.
2024 – The American Academy of Orthopaedic Surgeons updated its Management of Carpal Tunnel Syndrome clinical practice guideline in 2024. The guideline supports use of CTS-6 as a diagnostic tool and places structured clinical assessment ahead of routine ultrasound or electrodiagnostic testing in typical adult CTS presentations. Ultrasound or nerve conduction studies remain useful when diagnosis is uncertain, presentation is atypical, severity grading is needed, or preoperative clarification is required.
Summary
| Category | Tests / tools | Best use |
|---|---|---|
| Provocative symptoms | Hoffmann–Tinel, Phalen, reverse Phalen, Gilliatt–Wilson, Durkan, pressure provocative test | Reproduce median nerve symptoms |
| Symptom localisation | Katz–Stirrat hand diagram | Map symptom distribution |
| History clue | Flick sign | Relief by shaking/flicking hand |
| Sensory impairment | Semmes–Weinstein, two-point discrimination, vibration | Document sensory loss |
| Motor / functional impairment | Thumb abduction, Kapandji opposition, Moberg pick-up, Jamar grip | Grade severity and recovery |
| Patient-reported outcome | Boston / Levine questionnaire | Symptom and function scoring |
| Prediction tools | Wainner CPR, CTS-6 | Structured clinical diagnosis |
Associated Persons
- Sir James Paget (1814-1899)
- James Jackson Putnam (1846–1918)
- Charles Foix (1882–1927)
- Pierre Marie (1853–1940)
- Paul Hoffmann (1884-1962) and the Hoffmann-Tinel test
- Jules Tinel (1879-1952) and the Hoffmann-Tinel test
- George S. Phalen (1911-1998) and the Phalen test
- John A Durkan and the Durkan test
References
Historical
- Putnam JJ. A series of cases of paresthesia, mainly of the hands, of periodical recurrence, and possibly of vaso-motor origin. Archives of Medicine (New York). 1880; 4: 147–162.
- Hunt, J.R. The thenar and hypothenar types of neural atrophy of the hand. Am J Med Sci. 1911; 141:224-241
- Hoffmann P. Über eine Methode, den Erfolg einer Nervennaht zu beurteilen. [Using a method to assess the success of a nerve attack] Medizinische Klinik, 1915; 11: 359-360
- Hoffmann P. Weiteres über das Verhalten frisch regenerierter Nerven und über eine Methode, den Erfolg einer Nervennaht frühzeitig zu beurteilen. Medizinische Klinik. 1915; 11: 856-858.
- Tinel J. Le signe du ‘fourmillement’ dans les lésions des nerfs périphériques. La Presse Médicale. 1915; 47: 388–389. [English translation: Kaplan EB The “tingling” sign in peripheral nerve lesions. 1972 [PDF]]
- Brain WR, Wright AD, Wilkinson M. Spontaneous compression of both median nerves in the carpal tunnel; six cases treated surgically. Lancet. 1947 Mar 8;1(6443-6445):277-82.
- Gilliatt RW, Wilson TG. A pneumatic-tourniquet test in the carpal-tunnel syndrome. Lancet. 1953 Sep 19;265(6786):595-7.
- Bechtol CO. Grip test; the use of a dynamometer with adjustable handle spacings. J Bone Joint Surg Am. 1954 Jul;36-A(4):820-4
- Moberg E. Objective methods for determining the functional value of sensibility in the hand. J Bone Joint Surg Br. 1958 Aug;40-B(3):454-76.
- Phalen GS. The carpal-tunnel syndrome. Seventeen years’ experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Joint Surg Am. 1966;48(2):211-228.
- Pryse-Phillips WE. Validation of a diagnostic sign in carpal tunnel syndrome. J Neurol Neurosurg Psychiatry. 1984 Aug;47(8):870-2
- Kapandji A. Cotation clinique de l’opposition et de la contre-opposition du pouce [Clinical test of apposition and counter-apposition of the thumb]. Ann Chir Main. 1986;5(1):67-73.
- Katz JN, Stirrat CR. A self-administered hand diagram for the diagnosis of carpal tunnel syndrome. J Hand Surg Am. 1990 Mar;15(2):360-3
- Durkan JA. A new diagnostic test for carpal tunnel syndrome. J Bone Joint Surg Am. 1991 Apr;73(4):535-8. Erratum in: J Bone Joint Surg Am 1992 Feb;74(2):311.
- Williams TM, Mackinnon SE, Novak CB, McCabe S, Kelly L. Verification of the pressure provocative test in carpal tunnel syndrome. Ann Plast Surg. 1992 Jul;29(1):8-11.
- Levine DW, Simmons BP, Koris MJ, Daltroy LH, Hohl GG, Fossel AH, Katz JN. A self-administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. J Bone Joint Surg Am. 1993 Nov;75(11):1585-92
- Radecki P. A gender specific wrist ratio and the likelihood of a median nerve abnormality at the carpal tunnel. Am J Phys Med Rehabil. 1994 Jun;73(3):157-62.
- Wainner RS, Fritz JM, Irrgang JJ, Delitto A, Allison S, Boninger ML. Development of a clinical prediction rule for the diagnosis of carpal tunnel syndrome. Arch Phys Med Rehabil. 2005 Apr;86(4):609-18.
- Graham B. The value added by electrodiagnostic testing in the diagnosis of carpal tunnel syndrome. J Bone Joint Surg Am. 2008 Dec;90(12):2587-93.
Reviews
- Buch-Jaeger N, Foucher G. Correlation of clinical signs with nerve conduction tests in the diagnosis of carpal tunnel syndrome. J Hand Surg Br. 1994 Dec;19(6):720-4
- Szabo RM, Slater RR Jr, Farver TB, Stanton DB, Sharman WK. The value of diagnostic testing in carpal tunnel syndrome. J Hand Surg Am. 1999 Jul;24(4):704-14.
- D’Arcy CA, McGee S. The rational clinical examination. Does this patient have carpal tunnel syndrome? JAMA. 2000 Jun 21;283(23):3110-7.
- Paget J. The first description of carpal tunnel syndrome. J Hand Surg Eur Vol. 2007 Apr;32(2):195-7.
- Westerman D, Kerkhoff H, Visser GH, Kleyweg RP. Interobserver agreement in case history evaluation in carpal tunnel syndrome. J Clin Neuromuscul Dis. 2012 Jun;13(4):196-200
- McGee S. Evidence-Based Physical Diagnosis. 4e. 2017: 1196
- Genova A, Dix O, Saefan A, Thakur M, Hassan A. Carpal Tunnel Syndrome: A Review of Literature. Cureus. 2020 Mar 19;12(3):e7333.
- Kuschner SH, Lane C, Williams E. Comments on the Article “Grip Strength Measurement for Outcome Assessment in Common Hand Surgeries”: To the Editor. Clin Orthop Surg. 2022 Sep;14(3):474-475.
- Shapiro LM, Kamal RN; Management of Carpal Tunnel Syndrome Work Group; American Academy of Orthopaedic Surgeons. American Academy of Orthopaedic Surgeons/ASSH Clinical Practice Guideline Summary Management of Carpal Tunnel Syndrome. J Am Acad Orthop Surg. 2025 Apr 1;33(7):e356-e366.
eponymictionary
the names behind the name

Studying for Bachelor of Science (Occupational Therapy) at Curtin University
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |