
![]()
CT Case 108
A 50 year old male presents with 6 days of left lower quadrant abdominal and groin pain on a background of a left inguinal hernia repair 3 months ago.
He has no obstructive or infective symptoms. His exam reveals a soft abdomen with mild tenderness around his left lower quadrant and normal bowel sounds.
A CT of his abdomen is performed.
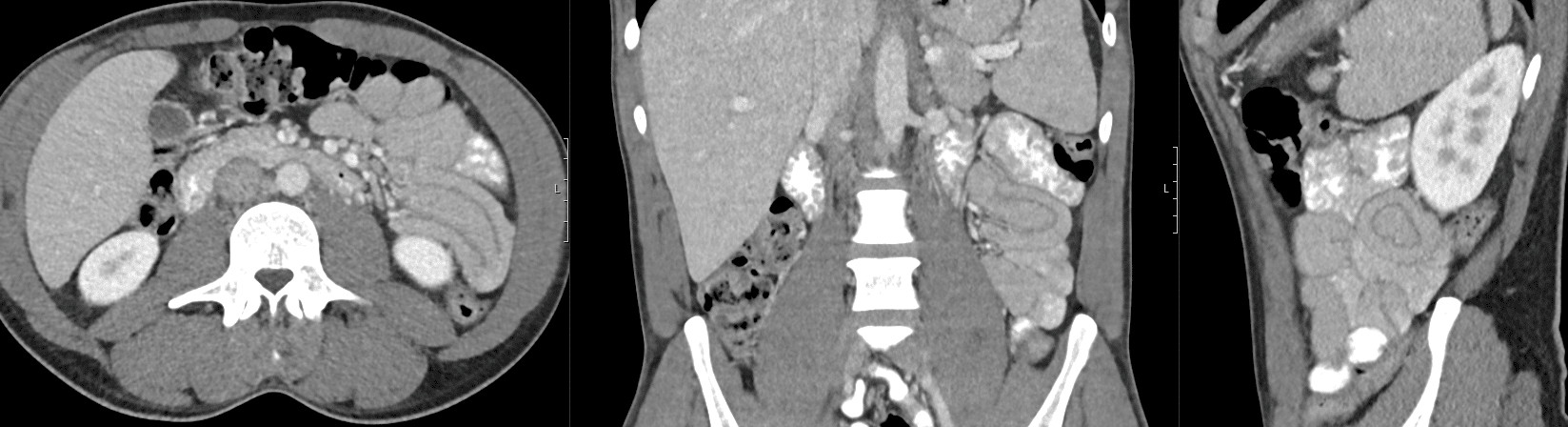
Describe and interpret the CT scan
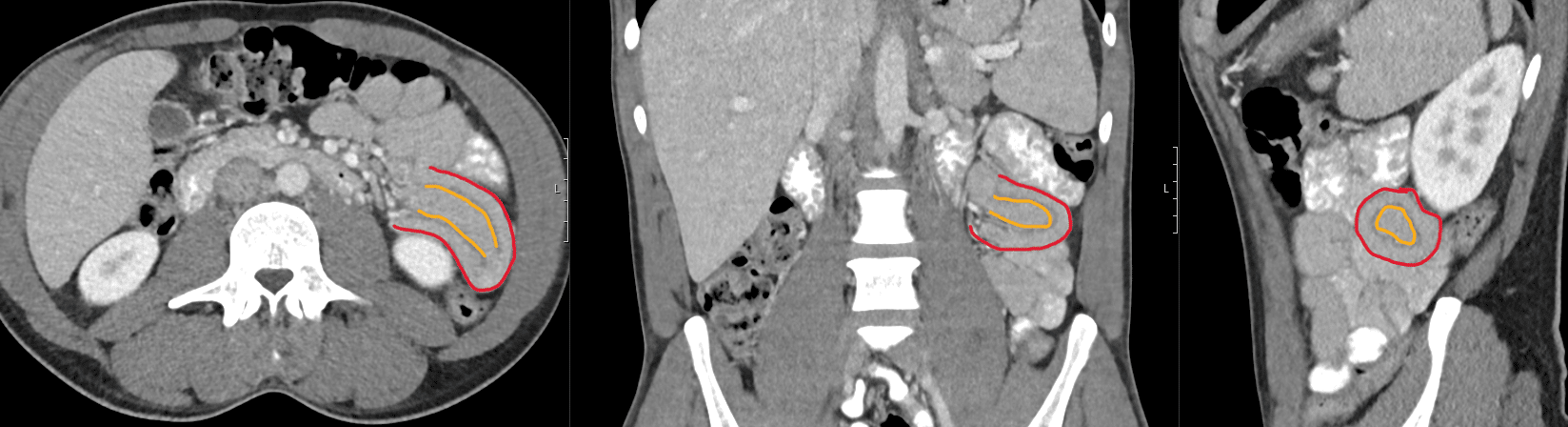
There is intussusception in the left upper quadrant involving the jejunum loops in a length of 5.7 cm without underlying lead point.
There is no bowel obstruction.
No evidence of bowel wall oedema or mesenteric stranding.
No evidence of free fluid .
Clinical Pearls
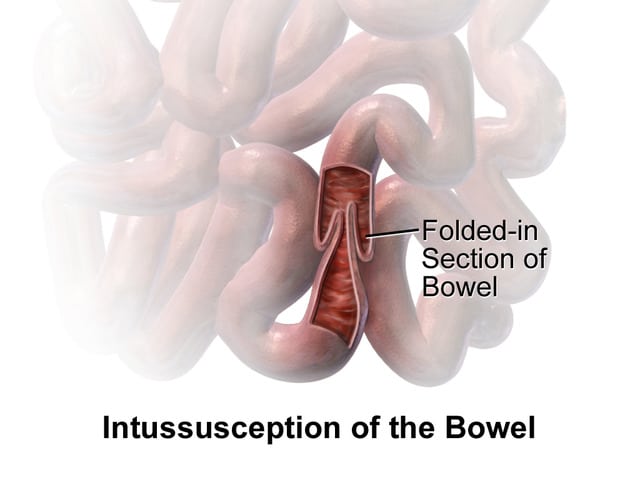
This patient has a jejuno-jejunal intussusception.
Intussusception is the invagination of a part of the intestine into itself. The most common location of intussusception occurs at the ileocecal junction (1). If left untreated these lesions may lead to bowel obstruction, ischaemia, and perforation.
A lead point is found in only 25% of cases. This is a lesion that is trapped by peristalsis and results in invagination of bowel into itself. There are several causes of lead points including Meckel diverticulum, polyps, cysts, tumours, haematomas, and vascular malformation (3). Lead points are more commonly found in adults compared to children, with neoplasm being the most common lead point in adults (4).
The peak incidence of intussusception is in young children between 4 and 36 months of age (2) and is a rare but often missed diagnosis in adults. Children usually present with abdominal pain and vomiting, and may develop a sausage-shaped mass palpable in the right lower quadrant of their abdomen. Bloody stools with a jelly-like appearance is classically described, but this is a late finding as it caused by mucosal sloughing and gross bleeding. Intussusception is the leading cause of bowel obstruction in this population.
Adults often present with vague symptoms such as abdominal pain, nausea, and constipation; only 1-5% of mechanical bowel obstructions in adults are due to intussusception (5).
Small bowel intussusception is sometimes found incidentally on CT, and the majority of these cases are transient and have little clinical significance. These episodes can be managed with observation alone if they are of short duration and have minimal symptoms. Follow up imaging may be obtained to confirm resolution where there are concerns of a lead point or bowel obstruction.
Treatment is guided by the location of the intussusception and the clinical stability of the patient. Non operative reduction with hydrostatic or pneumatic enema is the preferred treatment modality for children with ileocolic lesions who are stable. Surgery (reduction +/- bowel resection) is reserved for unstable patients, those with intestinal perforations, or where non operative reduction has been unsuccessful.
This patient was thought to have neuropathic abdominal pain caused by his recent inguinal hernia repair. The CT finding of an intussusception was thought to be an incidental finding due to the lack of obstructive symptoms and the clinical site of pain not matching the radiological site of intussusception. He was discharged with an outpatient MRI arranged to further assess the lesion.
References
- Mandeville K, Chien M, Willyerd FA, Mandell G, Hostetler MA, Bulloch B. Intussusception: clinical presentations and imaging characteristics. Pediatr Emerg Care. 2012 Sep;28(9):842-4.
- Yap Shiyi E, Ganapathy S. Intussusception in Children Presenting to the Emergency Department: An Asian Perspective. Pediatr Emerg Care. 2017 Jun;33(6):409-413.
- Lin XK, Xia QZ, Huang XZ, Han YJ, He GR, Zheng N. Clinical characteristics of intussusception secondary to pathologic lead points in children: a single-center experience with 65 cases. Pediatr Surg Int. 2017 Jul;33(7):793-797.
- Newsom BD, Kukora JS. Congenital and acquired internal hernias: unusual causes of small bowel obstruction. Am J Surg. 1986 Sep;152(3):279-85.
- Marinis A, Yiallourou A, Samanides L, Dafnios N, Anastasopoulos G, Vassiliou I, Theodosopoulos T. Intussusception of the bowel in adults: a review. World J Gastroenterol. 2009 Jan 28;15(4):407-11.
TOP 100 CT SERIES

FACEM, MBBS (Hon), B. Pharm. Emergency Medicine Education Fellow at Liverpool Hospital, Australia. Special interests in clinical education, ECG interpretation and diagnostic ultrasound. Proud father and husband, sadly a golf tragic

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney
