
![]()
Devil’s Horn Sign
aka Bone and Joint Bamboozler 005
A 22 year-old male injured his right hand as shown in the image below:

Describe and interpret the clinical image.
Bamboozler Answer
Description:
- Both hands are making the ‘devil’s horn’ sign well known to heavy metal aficionados.
- The finger positions are slightly different on the right hand compared with the left. The middle and ring fingers are not as completely flexed at the metacarpophalangeal joints and the little finger is not completely extended.
- There is an open wound on the dorsum of the right hand overlying the proximal 5th metacarpal, with a white structure protruding from, or visible within, the wound.
- There are other superficial wounds overlying the metacarpophalangeal joints and phalanges on the dorsum of the middle, ring and little ringers of the right hand.
Interpretation:
- The findings are consistent with a ZONE 6 extensor tendon injury of the right hand, affecting extensor digiti minimi.
- The white structure seen within the wound is the transected tendon.
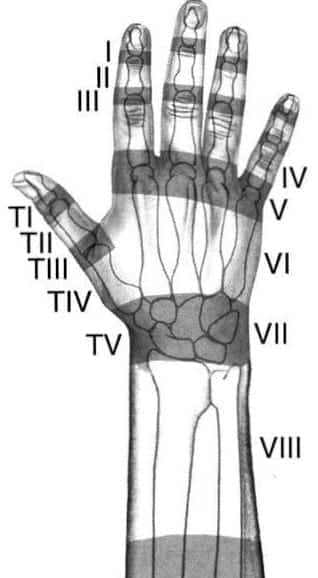
What are the zones of the hand?
Bamboozler Answer
These zones are worth knowing as the anatomic location of extensor tendon injuries influences treatment.
Zone 6 extensor tendon injuries may occur with seemingly trivial skin wounds as the tendons are very superficial in this region.
Any wound in Zone 6 involves a tendon injury until proven otherwise!
Why are these injuries potentially difficult to detect clinically?
Bamboozler Answer
It is easy when the severed tendon is on view!
Always move the nearby joints through full range of motion when assessing a wound to ensure tendon injuries aren’t missed.
Depending on the position of the hand at the time of injury, the site of tendon injury may be distant from the wound at the time of examination.
Extensor tendons of the 2nd to 5th digits of hand are connected by the juncturae tendini (fibrous bands passing obliquely between the diverging tendons of the extensor digitorum and extensor digiti minimi on the dorsum of the hand) near the metacarpophalangeal joints, as shown below.
Extensor tendon injuries proximal to these connections can be missed because the affected digit can still be extended (with less strength) by the action of the adjacent extensor tendon transmitting force through the juncturae tendini.
To detect functional impairment from these injuries test active extension of the affected digit with the other digits flexed at the metacarpophalangeal joints.
For the little finger, and presumably the index finger too, this can also be done by performing the ‘devil’s horn’ sign!
The full story of the patient in the photo is enlightening in this respect:
Whilst partying with some friends he fell over in some sand, cutting his right hand on some buried glass. He washed the wound out and wasn’t too worried about the injury – even though the severed tendon was visible – because his hand seemed to work just fine. It was only later, when he turned up the Metal on the stereo, that he attempted the ‘Devil’s Horn’ sign and realized that his little finger didn’t extend properly…

How is this injury managed?
Bamboozler Answer
Management overview:
- Exclude/ treat other injuries (e.g. secondary survey; x-ray to rule out fractures and radio-opaque foreign bodies)
- Analgesia
- Update tetanus immunization if appropriate
- Consider antibiotics (unproven, but often given if contaminated, delayed presentation or admission for delayed closure)
- Clean, explore and irrigate the wound
- Zone 6 extensor tendon injuries can usually be repaired by a figure-of-eight stitch (or similar technique) using 4-0 non-absorbable sutures and a straight needle.
- Following repair the hand should be splinted with the wrist at 30 degrees extension and the MCPJs in neutral position. Roberts and Hedges suggest a dorsal slab with malleable metal and foam extension to splint the affected finger.
- Early follow up with a hand specialist should be arranged (e.g <1 week)

Can definitive treatment occur in the ED?
Bamboozler Answer
Extensor tendon ruptures may be repaired in the ED in specific circumstances (mostly from Trott, 2005):
- if the injury is between the distal wrist and the metacarpophalangeal joints (zone VI)
- if the skin and tendon wounds are sharp and not heavily macerated or contaminated
- if the injury is less than 8 hours old
- if the two ends of the tendon are easily visualized
- if appropriate instruments are available to minimize trauma to the tissues
- if a doctor/ surgeon is available with the appropriate training and experience
- if the patient is cooperative and will comply with follow-up care
- if in accordance with local standards of practice
In our case, the injury was about 20 hours old so the patient was admitted for IV antibiotics pending further wound washout and tendon repair by an orthopedic surgeon in an operating theatre.
References
- Griffin M, Hindocha S, Jordan D, Saleh M, Khan W. Management of extensor tendon injuries. Open Orthop J. 2012;6:36-42. Epub 2012 Feb 23. [PMID 22431949];
- Rosen’s Emergency Medicine 8th edition
- Roberts and Hedges’ Clinical Procedures in Emergency Medicine, 6e
- Trott, AT. Wounds and Lacerations Emergency Care and Closure
- Butterfly Language – Is the Sign of the Horns Hand Gesture Satanic?
- Sherman, S. Simon’s Emergency Orthopedics 7e
- Purcell, D. Minor Injuries A Clinical Guide 3e
CLINICAL CASES
Bone and Joint Bamboozler
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
Oh my this made my day!! I will never forget the “devil’s horn sign”…hahaha