
![]()
Echo basics: Measurements and Reports
Assessment of heart valve structure and function
A comprehensive evaluation of valvular heart disease relies on accurate measurements derived from both two-dimensional (2D) imaging and Doppler waveforms. These measurements are essential for quantitative analysis and for guiding clinical decision-making.
Two-Dimensional Imaging
- Image optimization is critical: use zoom, image gain adjustment, and probe angulation to achieve the clearest possible views.
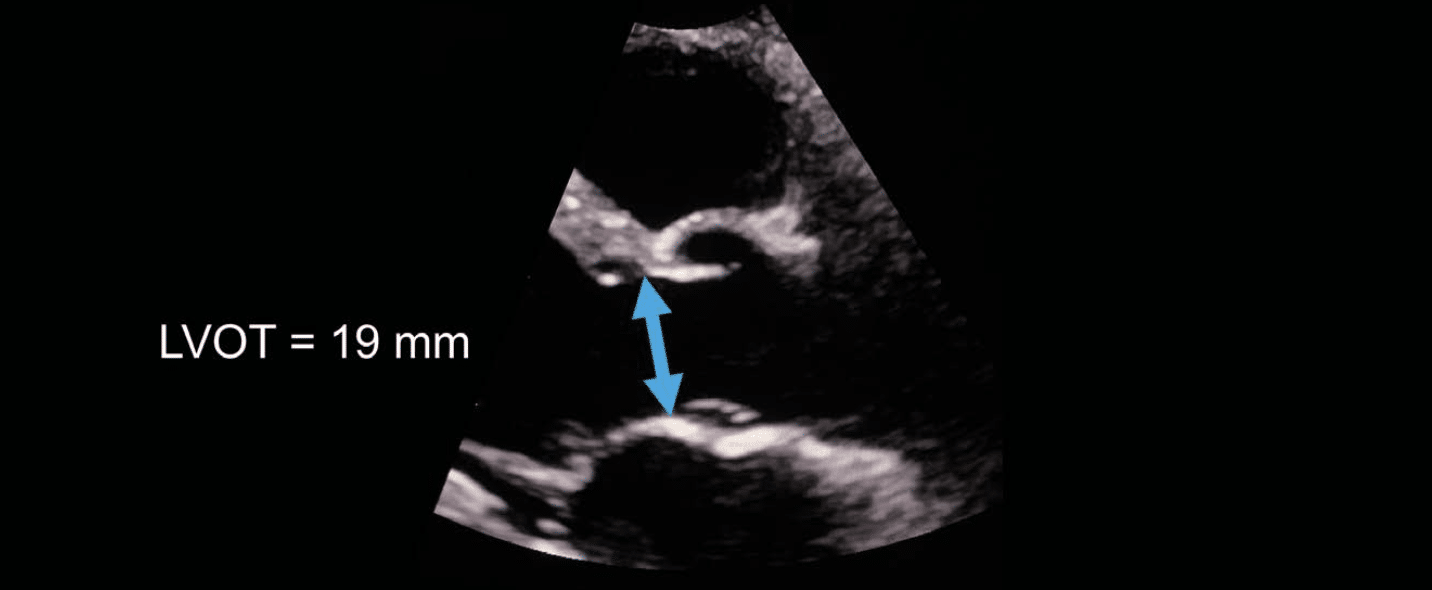
- LVOT diameter should be measured routinely:
- Use a zoomed parasternal long-axis view
- Measurement is made inner edge to inner edge
- Performed at the base of the aortic valve cusps during mid-systole
Doppler Techniques
General Principles
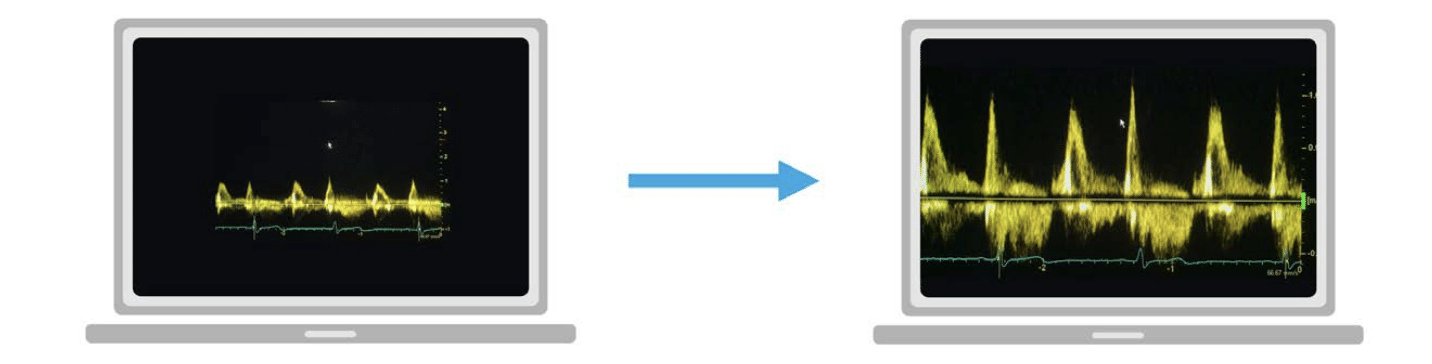
- Velocity scales should be adjusted so that the Doppler waveform fills the display, allowing for more accurate tracing and peak velocity determination.
Continuous Wave (CW) Doppler
- Used to measure high velocities (e.g., across stenotic valves).
- Ensure the Doppler cursor is aligned with the direction of blood flow.
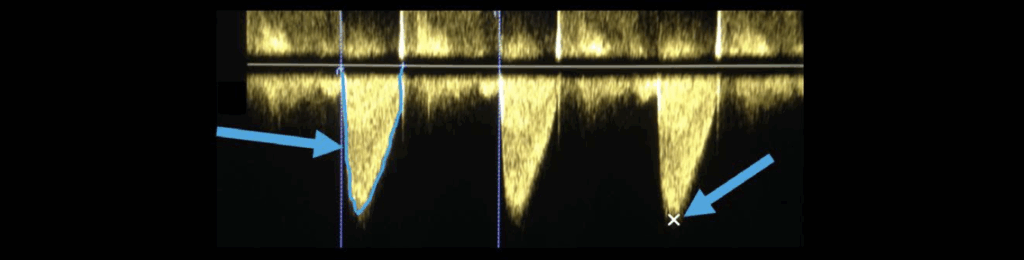
- Peak velocity: Place the cursor at the top of the densest part of the signal.
- Mean velocity: Trace around the full spectral envelope of the Doppler waveform.
Pulsed Wave (PW) Doppler
- Allows site-specific velocity assessment.
- Adjust the sample volume location until a clear, smooth velocity curve is visualized.
- Optimal trace characteristics:
- Clear closing click of the valve
- Less dense central waveform
- Avoid placing the sample too close to the valve (may show opening clicks)
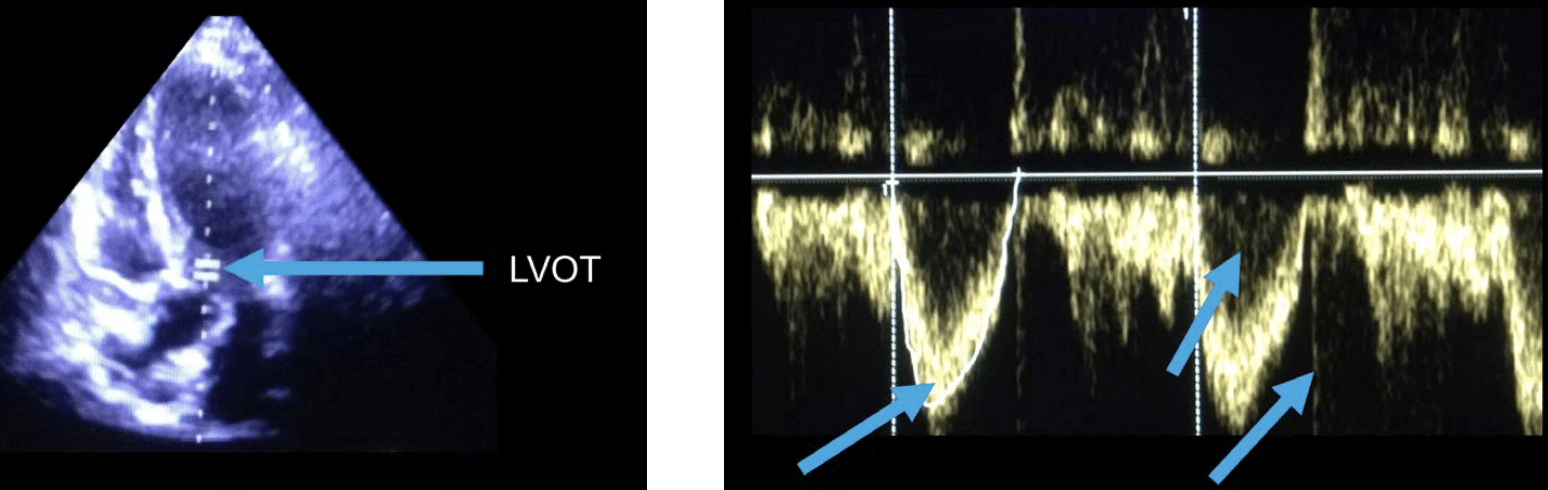
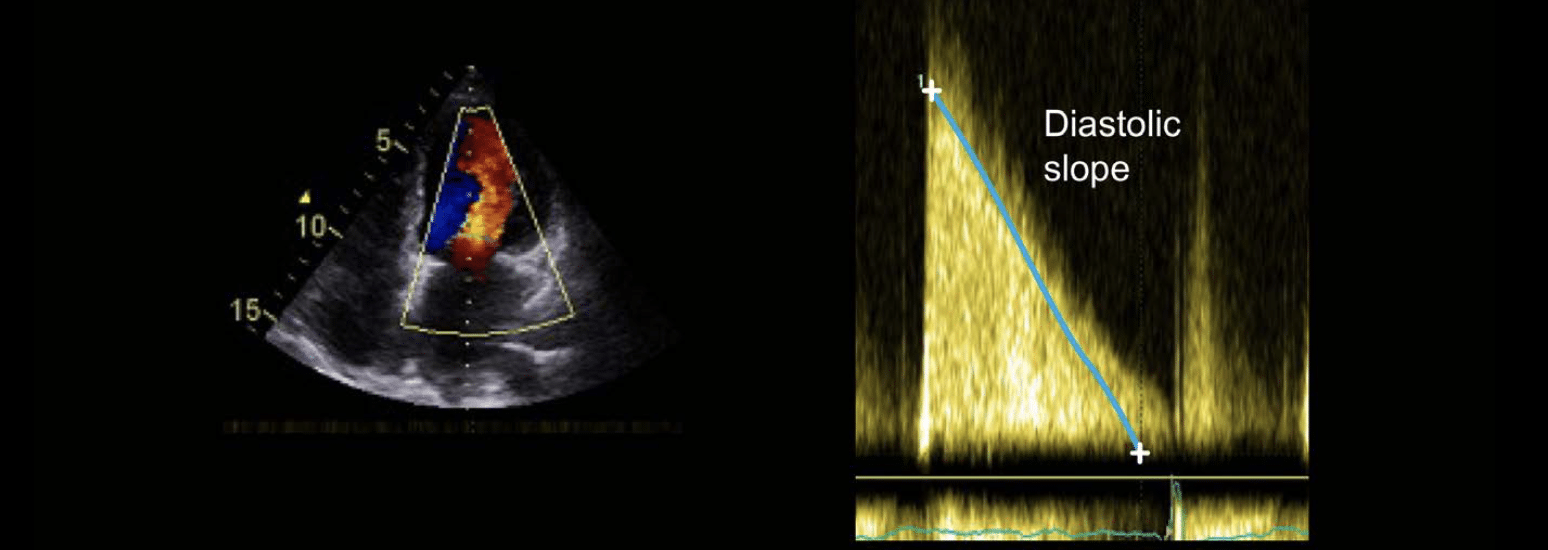
Pressure Half-Time (PHT)
- Used for mitral valve assessment, particularly in mitral stenosis.
- Place the PW Doppler sample volume at the tip of the mitral leaflets.
- Draw a line from the maximum velocity down the diastolic slope of the waveform.
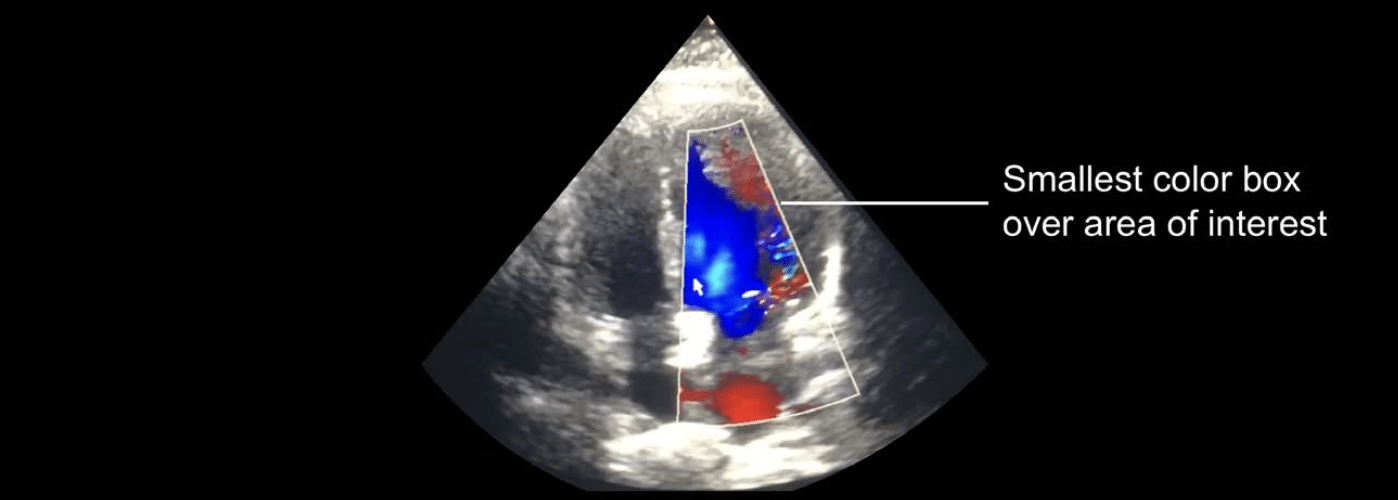
Color Doppler
- Box size: Use the smallest box necessary to cover the region of interest to maximize frame rate.
- Gain optimization:
- Increase gain until random speckle noise is seen
- Then reduce slightly until the speckle just disappears
Reporting in valve assessment
A comprehensive echocardiography report integrates all imaging findings to form the basis of clinical decision-making and patient management, especially in cases of valve disease.
General Principles
- The report should clearly describe what was observed during the echo study.
- Abnormal valves will often require more detailed descriptions.
- Integrate findings from multiple views and modalities (2D, Doppler, Color) for a concise, coherent explanation.
- All measurements should be included and referenced against normal ranges.
- An overall conclusion should:
- Be clear and concise
- Summarize the key abnormality
- Identify other relevant findings
- Be written in a style understandable by non-specialist staff
- Include a comparison to previous studies, if applicable
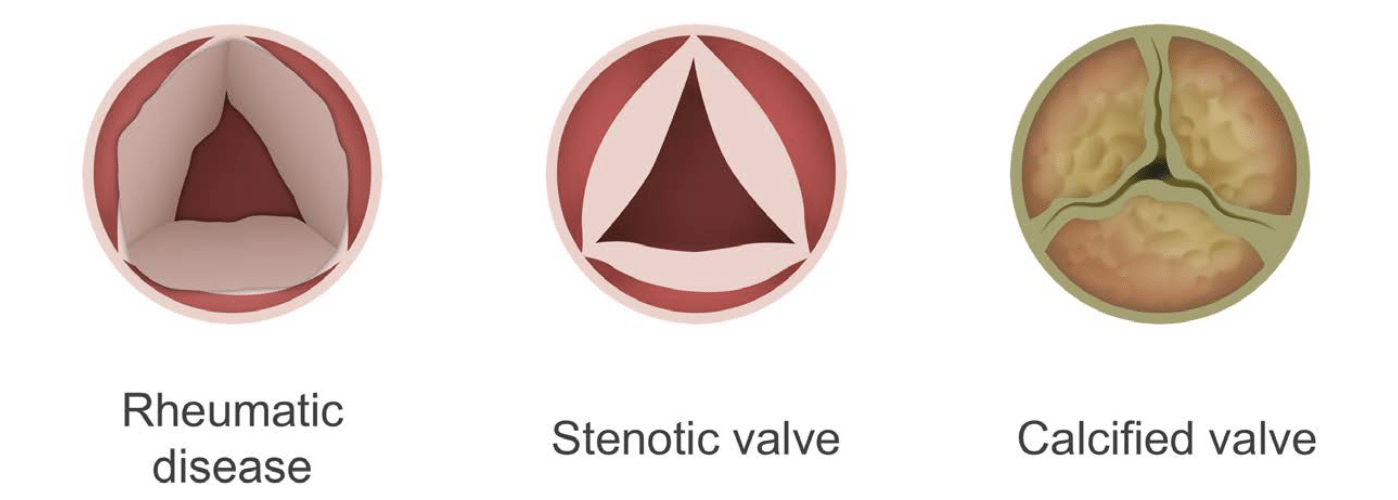
Reporting Valve Stenosis
When valve stenosis is identified, include the following details:
- Appearance of the valve (e.g. calcified, thickened, restricted mobility)
- Severity of stenosis (e.g. mild, moderate, severe based on Doppler parameters)
- Left ventricular (LV) dimensions and systolic function
- Assessment of subvalvular apparatus (especially in atrioventricular valves like the mitral and tricuspid)
- Function of other cardiac valves
- Right ventricular (RV) function and pulmonary artery pressure (PAP)
Reporting Valve Regurgitation
When valve regurgitation is present, include:
- Severity of regurgitation (qualitative and quantitative)
- Cause of regurgitation (e.g. prolapse, annular dilation, leaflet perforation)
- LV and aortic root dimensions
- LV systolic function
- Function of other valves
- RV function and pulmonary artery pressure
Reporting Prosthetic Valves
For patients with prosthetic heart valves, include:
- Valve type and position (e.g. mechanical mitral, bioprosthetic aortic)
- Any signs of obstruction (e.g. high velocity, restricted leaflet motion)
- Doppler flow measurements through the valve
- Severity and source of any regurgitation (e.g. transvalvular vs paravalvular)
- LV dimensions and function
This is an edited excerpt from the Medmastery course Echo Masterclass – The Valves by Chris Eggett, PhD. Acknowledgement and attribution to Medmastery for providing course transcripts.
Additional echocardiography resources:
- Na, M. Echo Masterclass: Left Ventricular Strain. Medmastery
- Monteiro, C. Echo Masterclass: The Right Heart. Medmastery
- West, C. Echo Masterclass: Adult Congenital Heart Disease. Medmastery
- Naderi, H. Echo Masterclass: The Power of 3D Imaging. Medmastery
Radiology Library: Echocardiography basics
- Eggett C. Echo basics: Valve Views. LITFL
- Eggett C. Echo basics: Valves, Measurements and Reports. LITFL
- Eggett C. Echo basics: Mitral valve. LITFL
- Eggett C. Echo basics: Mitral Regurgitation. LITFL
- Eggett C. Echo basics: Mitral Stenosis. LITFL
- Eggett C. Echo basics: Aortic Valve. LITFL
- Eggett C. Echo basics: Aortic Stenosis. LITFL
- Eggett C. Echo basics: Aortic Regurgitation. LITFL
- Eggett C. Echo basics: Tricuspid Valve. LITFL
- Eggett C. Echo basics: Pulmonary Valve. LITFL
- Eggett C. Echo basics: Prosthetic Valves. LITFL
Further reading
- Otto CM. Textbook of Clinical Echocardiography. Elsevier. 7e, 2023.
- Houghton AR. Making Sense of Echocardiography: A Hands-on Guide. 3e 2023
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM 3rd, Thomas JD; ACC/AHA Task Force Members. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Jun 10;129(23):e521-643
Echocardiography Essentials

Cardiac physiologist, echocardiographer, and Professor of Healthcare Science Education, Faculty of Medical Sciences at the University of Newcastle, UK. I direct post-grad programs at the Faculty of Medical Sciences, run an echo clinic at the Freeman Hospital, and teach transthoracic echocardiography to specialists in critical and emergency care and anaesthetic settings