
![]()
Edward Bishop

Edward Harry Bishop (1913-1995) was an American obstetrician and gynecologist
Author of 50 original research articles, principally concerning Doppler ultrasonic fetal monitoring, intrauterine transfusion, management of premature labor, cesarean section mortality, acceleration of fetal pulmonary maturity with steroids, induction of labor, and the quality of perinatal care in North Carolina, and induction of labor.
Bishop was one of the first physicians to treat the fetus with an intrauterine transfusion and one of the first obstetricians to deal with genetic diagnosis of the fetus.
Eponymously remembered for the Bishop Score (1964), a method to evaluate the cervix in regard to the success or failure of induction of labor.
Biography
- Born on June 13, 1913 in Bethlehem, New Hampshire
- 1937 – MD, Dartmouth College and Medical School
- Completed training in obstetrics and gynecology at the Methodist Hospital in Philadelphia
- 1967-1970 Chairman of the Committee on Maternal Health for the American College of Obstetricians and Gynecologists
- 1971 – Professor of Obstetrics and Chief of Perinatology at the University of North Carolina (UNC) School of Medicine in Chapel Hill
- 1974-1979 First Chief of the Division of Maternal–Fetal Medicine, UNC
- 1982 – Retired
- Died on December 10, 1995
Medical Eponyms
Bishop Score (1964)
The Bishop Score is a schematic method used to estimate the likelihood of imminent delivery in a pregnant woman based on what degree her cervix is prepared for labor. These factors include the degree of cervical dilation, effacement, consistency, position, and the station of the presenting part. This calculated pelvic score holds value in determining the optimal time for elective induction.
1955 – Bishop described the optimal factors for elective induction of labor in pregnant patients.
In the 1950s, synthetic oxytocin came to use as a method for elective induction of labor. During this time, Bishop and the Obstetrics and Gynaecology staff at Pennsylvania hospital became interested in methods to improve the effectiveness of inducing labor.
From December 1951 to September 1954, Bishop analysed 1,000 elective inductions of labor at the hospital of Pennsylvania, an incidence of 0.8% of all the births during this time.
Bishop found no significant difference between the methods used to initiate induction of labor, and instead, recognised the significance of a woman’s pelvic factors contributing to the effectiveness of an induction of labor.
The success of elective induction of labor was determined by the length of labor, from initiation of induction to the end of the third stage of labor, and the factors contributing to the success were described by Bishop.
The results [of elective induction of labor] are most satisfactory when induction is limited to multiparous patients with the presenting part a station minus 1 or lower, and with the cervix not less than 60 per cent effaced and not less than 3cm dilated.
Induction of labor under less favorable circumstances may be successful, but this is associated with an increased incidence of long labors. Elective induction of labor is an acceptable procedure when limited to those patients who fulfil the most favorable criteria
Bishop EH. Elective Induction of Labor. 1955
1964 – Bishop described a pelvic scoring system, the ‘Bishop Score’, to estimate the expected date of delivery of a foetus, and to determine the optimal time for elective induction of labor.
In the 1960s elective induction of labor became increasingly common. Proponents claimed a short, easy, and convenient labor is associated with minimal and acceptable perinatal mortality. Others condemned the practice as dangerous, incurring an unnecessary risk to both the mother and her child.
Bishop determined that differences in results arose from variations in the method of selecting suitable candidates. In 1964 he presented his method of selecting suitable candidates for elective induction of labor.
Bishop maintained from his previous study in 1955, that induction should only be considered in cases of multiparity; >36 weeks gestation; vertex presentation; normal previous and present obstetric history; and advance knowledge and permission of the patient.
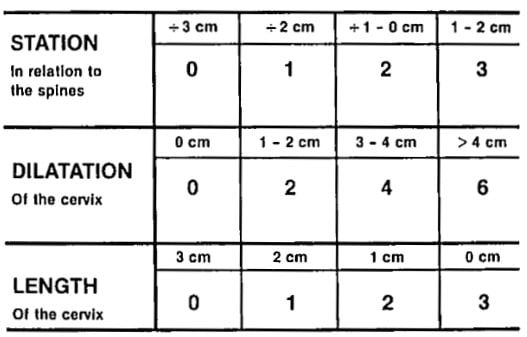
…determination of suitability for elective induction is made by evaluation of certain pelvic factors which usually presage the spontaneous onset of labor. Such factors are dilatation, effacement, consistency, and position of the cervix, and the station of the presenting part.
…one may estimate the expected date of delivery more accurately than by the traditional methods. Such a scoring system is of extreme value in determining the optimum time for elective induction of labor and for elective repeat cesarean section. Scores which appear unrelated to the expected date of delivery may forewarn the obstetrician of the possibility of either premature labor or postmaturity
Bishop EH. Pelvic scoring for elective induction, 1964

1982 – Lange et al., published Prelabor Evaluation of Inducibility in 1982, proposing a new cervical scoring system to be used in the prelabour evaluation of inducibility – the Modified Bishop Score
The influence of cervical dilatation on the Bishop pelvic score should be weighed twice as high as station, effacement, and consistency, while position should only be weighted half its present influence.
The consistency and position of the cervix have been omitted, and the station of the presenting part of the fetus and length of the cervix are unchanged [from the original Bishop score].
In the study conducted, there were some difficulties in interpreting the data as only successful cases were included in the study and primary artificial rupture of membranes was performed in almost all the cases analysed
Clinical Use of the Bishop Score
The Bishop Score is commonly used in medical practice today, to predict the likelihood of a successful vaginal delivery, and the need for a caesarean section after the onset of labor or induction.
There is no universally accepted definition of a favourable or unfavorable cervix, however, most obstetricians consider a score ≥7 to be favourable.
Some institutions recommend using the Modified Bishop Score (1982), as an update to Bishop’s original scoring system (1964).
Before the induction of labor in a pregnant woman, the modified bishop score may be used to determine the use of cervical ripening, recommended with a modified bishop score of <8. If the modified bishop score ≥ 7 (favourable) then induction of labor may proceed without cervical ripening.
Key Medical Contributions
Uterine Tocolysis (1961)
Bishop was one of the first to attempt uterine tocolysis with isoxsuprine.
In April of 1961, Edward Bishop and Theodore Woutersz conducted a preliminary two-phase trial to attempt tocolysis with isoxsuprine. The pair determined that isoxsuprine is effective to arrest uterine contractions in most premature labors.
By November of 1961, the pair published ‘Arrest of Premature Labor’, continuing their study of isoxsuprine in the arrest of premature labor.
Following isoxsuprine therapy, premature uterine contractions ceased for a significant period of time in 66 per cent of the cases studied, and labor did not recur until the fetal weight had reached a minimum of 2500g, in 42% of patients.
Bishop 1961
These findings contributed significantly to obstetrics reducing the incidence of preterm deliveries and the associated mortality associated with a pre-term infant.
Doppler Ultrasound (1966)
Bishop was involved in the early development of Doppler ultrasound monitoring of the fetal heart. He described the Doptone Doppler ultrasonic motion sensor developed by Smith Kline Instrument Company, Pennsylvania in 1966.
This instrument allowed practitioners to demonstrate fetal blood flow after 12-13weeks gestation, and some as early as 10 weeks. A major innovation from the previous use of a fetoscope which did not allow the fetal heart to be heard until 16 weeks gestation at the earliest.
Major Publications
- Bishop EH. Elective Induction of Labor. Obstet Gynecol 1955; 5(4): 519–27.
- Bishop EH, Woutersz TB. Isoxsuprine, a Myometrial Relaxant: A Preliminary Report. Obstet Gynecol 1961; 17(4): 442–6.
- Bishop EH, Woutersz TB. Arrest of premature labor. JAMA. 1961 Nov 25;178:812-4.
- Bishop EH. Pelvic scoring for elective induction. Obstet Gynecol. 1964 Aug;24(2):266-8
- Bishop EH, Buston CL. Prematurity. 1964
- Bishop EH. Instrument and method: the Doppler ultrasonic motion sensor. Obstet Gynecol 1966; 28(5): 712–3.
- Bishop EH, Guinto FC. Amniography. 1973
- Bishop EH. Elective induction of labor. 1973
- Bishop EH, Bishop DE. Perinatal medicine: practical diagnosis and management. 1982
- Bishop EH, Cefalo RC. Signs and symptoms in disorders of pregnancy. 1983
References
Biography
- Powell JL. Powell’s pearls: Edward Harry Bishop, MD (1913-1995). Obstet Gynecol Surv. 2006 Jul;61(7):425-6.
- Cefalo RC. Edward H. Bishop, M.D. American Gynecological Obstetrical Society.
- Baskett TF. Bishop, Edward Harry (1913–1995) In: Eponyms and Names in Obstetrics and Gynaecology. 3e. 2019: 41-42
- Bibliography. Bishop, Edward H. WorldCat Identities
Eponymous terms
- Lange AP, Secher NJ, Westergaard JG, Skovgård I. Prelabor evaluation of inducibility. Obstet Gynecol. 1982 Aug;60(2):137-47.
- Vrouenraets FP, Roumen FJ, Dehing CJ, van den Akker ES, Aarts MJ, Scheve EJ. Bishop score and risk of cesarean delivery after induction of labor in nulliparous women. Obstet Gynecol. 2005 Apr;105(4):690-7.
- Laughon SK, Zhang J, Troendle J, Sun L, Reddy UM. Using a simplified Bishop score to predict vaginal delivery. Obstet Gynecol. 2011 Apr;117(4):805-811.
- Teixeira C, Lunet N, Rodrigues T, Barros H. The Bishop Score as a determinant of labour induction success: a systematic review and meta-analysis. Arch Gynecol Obstet. 2012 Sep;286(3):739-53.
- Kolkman DG, Verhoeven CJ, Brinkhorst SJ, van der Post JA, Pajkrt E, Opmeer BC, Mol BW. The Bishop score as a predictor of labor induction success: a systematic review. Am J Perinatol. 2013 Sep;30(8):625-30.
- Abboud CJ. Pelvic Scoring for Elective Induction. Embryo Project Encyclopedia (2017-02-23)
Eponym
the person behind the name

Doctor at King Edward Memorial Hospital in Western Australia. Graduated from Curtin University in 2023 with a Bachelor of Medicine, Bachelor of Surgery. I am passionate about Obstetrics and Gynaecology, with a special interest in rural health care.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |