
![]()
Foreign body pulmonary embolisation
Migration of a subdermal contraceptive implant to the pulmonary artery
A 36-year-old woman presented with new irregular menstrual bleeding. An Implanon NXT device had been inserted into the medial aspect of her left upper arm 14 months earlier, after which she had experienced amenorrhoea. For the preceding month, she had been unable to palpate the implant and was concerned that it was no longer in situ.
On examination, she was haemodynamically stable and systemically well. The implant was not palpable in the left upper arm. Ultrasound of the left upper arm failed to identify the device.
A chest X-ray was performed to assess for distant migration and demonstrated a very subtle linear radiopaque foreign body projected over the right lower lung field (drag the slider to reveal the annotated finding)


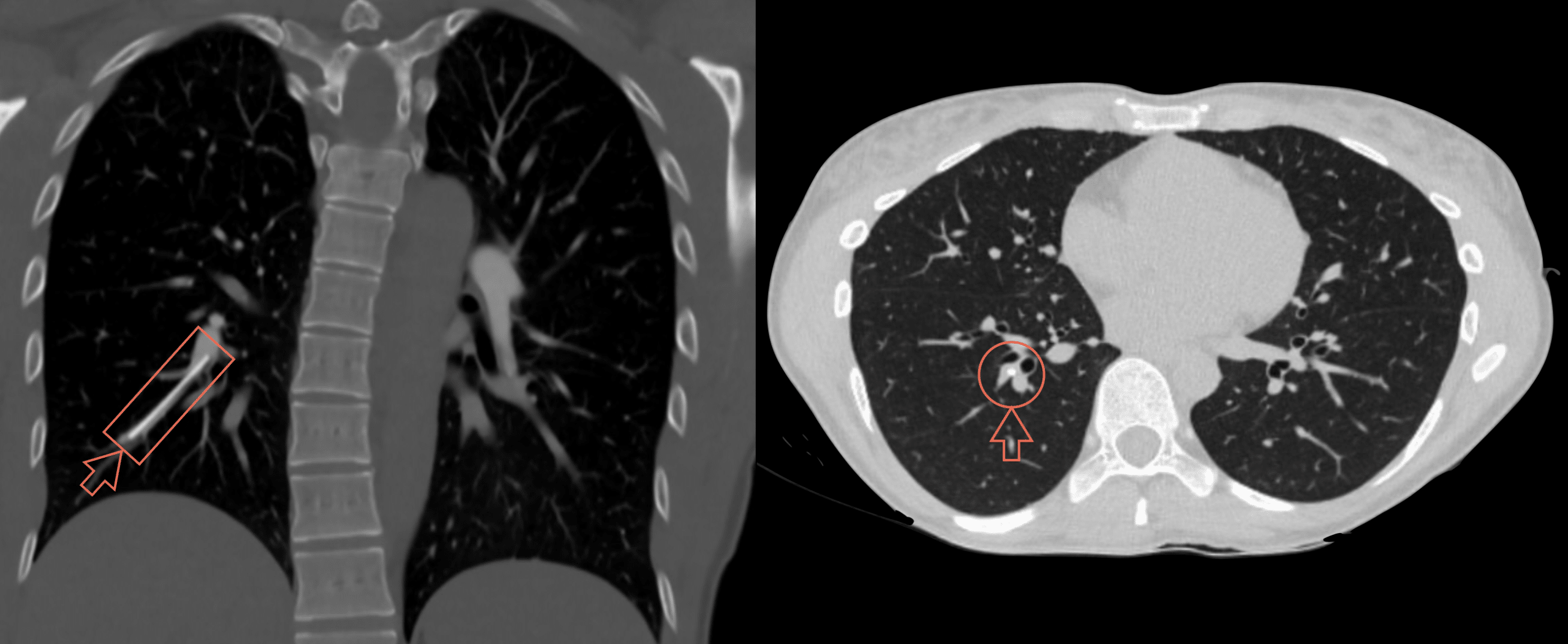
Subsequent CT pulmonary angiography confirmed a 4 cm linear hyperdense foreign body within the right pulmonary arterial tree, consistent with embolisation of the Implanon NXT device.
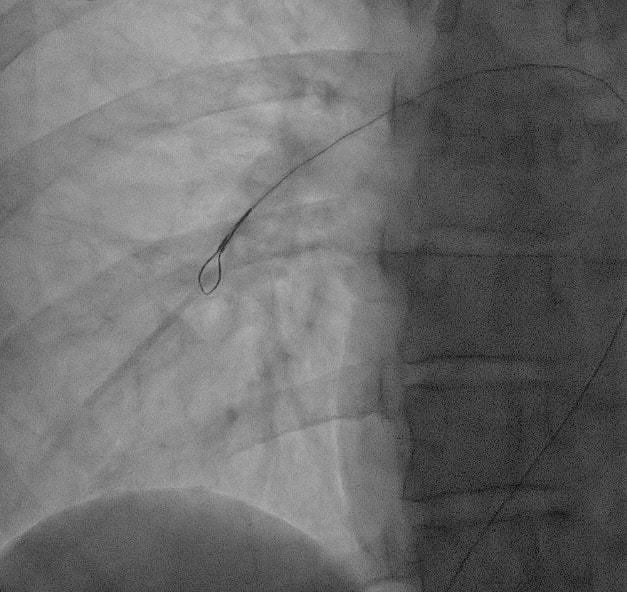
The implant was subsequently retrieved under fluoroscopic guidance by endovascular technique.
Pulmonary arterial embolisation of a contraceptive implant Q/A
1. What was the first clue?
A contraceptive implant that was expected to remain palpable in the upper arm can no longer be felt by the patient or clinician. In this case, new irregular bleeding prompted review, but the most important diagnostic clue was anatomical. The previously palpable implant in the left upper medial arm was no longer palpable.
2. What is the device?
Implanon NXT/Nexplanon is a small, flexible, 4 cm etonogestrel contraceptive rod designed for subdermal insertion in the upper arm. Unlike earlier non-radiopaque Implanon devices the Implanon NXT/Nexplanon contains barium sulphate, making it visible (radiopaque) on plain X-ray and CT. This allows a missing implant to be followed beyond the arm if local imaging fails to identify it.
3. Is this migration or embolisation?
Local implant migration refers to movement over a short distance from the insertion site. Pulmonary arterial migration requires access to the venous circulation, transit through the right heart, and lodgement in a pulmonary arterial branch. Once the implant reaches the pulmonary arterial circulation this process is more accurately described as intravascular foreign body embolisation.
4. How can a contraceptive implant inserted in the arm reach the pulmonary artery?
The most commonly proposed route is venous. If the implant enters an upper limb vein, it can pass through the axillary and subclavian venous system, enter the superior vena cava, pass through the right atrium and right ventricle, and lodge in the pulmonary arterial tree.
The commonly cited venous entry points are the basilic and brachial veins given their proximity to the medial upper arm insertion region. The exact point of venous entry is rarely proven in individual cases.
5. Did embolisation occur at insertion, or later?
Some published cases suggest primary intravascular placement, particularly if the implant was never palpable or insertion was followed by significant bleeding, bruising, or haematoma. Other cases are less clear, especially when the implant was reportedly palpable for weeks or months after insertion.
A key distinction is time to detection versus time to embolisation. A device discovered in the pulmonary artery months or years after insertion may have embolised early and remained clinically silent until attempted palpation, replacement, or removal.
6. How do patients present?
Many patients are asymptomatic. The problem is often discovered when the implant cannot be palpated at planned removal, replacement, or assessment of contraceptive efficacy. Others present with respiratory or chest symptoms, including chest pain, dyspnoea, cough, haemoptysis, non-specific chest discomfort, or rarely pneumothorax.
Symptoms do not reliably predict the location of the implant or whether endovascular retrieval will be possible.
7. How should a missing implant be investigated?
A non-palpable implant should be actively localised. The initial search should begin in the arm, with physical examination and local imaging. Ultrasound is commonly used and plain X-ray is useful for radiopaque devices.
If the implant is not identified in the upper limb, the search should extend to the chest. Chest radiography may demonstrate a subtle or obvious linear radiopaque foreign body projected over the lung field. CT pulmonary angiography should then be performed to confirm whether the device is intravascular, define the pulmonary arterial branch involved, assess how distal it lies, and look for associated thrombosis, stenosis, infarction, or parenchymal change.
8. Where does the implant lodge?
Published cases include right- and left-sided pulmonary arterial locations. Many implants lodge in lower-lobe segmental or subsegmental branches, but right upper lobe, right middle lobe, right lower lobe, left upper lobe and left lower lobe cases have all been described. The implant typically lodges distally in a segmental or subsegmental pulmonary arterial branch, rather than in one predictable lobe.
9. Why does timing matter?
Timing matters because a foreign body lodged in a pulmonary arterial branch may become endothelialised, fibrosed, encapsulated, or embedded in the vessel wall. Once this occurs, endovascular snare retrieval may fail or become hazardous. Attempted traction on a fixed implant risks vascular injury, bleeding, or incomplete retrieval.
Early localisation may therefore increase the chance of successful endovascular removal, while delayed diagnosis may require thoracoscopic or open surgical techniques.
10. How is it removed?
When feasible, endovascular retrieval is the least invasive option. Reported techniques include femoral or internal jugular venous access, pulmonary arteriography, catheter manipulation, and loop-snare retrieval.
If the implant is distal, fixed, endothelialised, or inaccessible, surgical management may be required. Reported approaches include thoracoscopic arteriotomy, mini-thoracotomy, wedge resection, and segmentectomy. In some patients, the implant has been left in situ because retrieval failed, was considered too risky, the device was thought to be hormonally inactive, or the patient declined intervention.
11. Does every pulmonary arterial implant need removal?
No universal rule exists. Management should be individualised according to symptoms, implant location, vascular compromise, evidence of thrombosis, duration since insertion, technical retrievability, ongoing hormonal activity, pregnancy wishes, procedural risk, and patient preference.
The long-term consequences of leaving a contraceptive implant within the pulmonary arterial system remain uncertain.
12. What is known about incidence and risk factors?
Pulmonary arterial embolisation of etonogestrel implants is rare, and its true incidence is uncertain. Data are limited by under-reporting, duplicate reporting, reporting bias, and increased detection after safety warnings.
The strongest suspected risk factor is insertion technique, particularly deep or intravascular insertion. Other proposed contributors include low body mass, thin arms, repeat insertion at the same site, insertion near mobile tissue planes or neurovascular structures, and subsequent local movement.
13. What do larger reports and reviews show?
The literature is difficult to summarise because it consists of overlapping case reports, pharmacovigilance datasets, national reporting studies and small management cohorts. Individual case reports are useful for mechanism and imaging appearances, drug surveillance datasets define epidemiology whilst management studies inform retrieval success and failure. The following table summarises key journal articles within these realms.
| Source | What was reviewed | What was found |
|---|---|---|
| Kang 2017 | FAERS pharmacovigilance 38 etonogestrel implant migrations, excluding cases already published in the literature | 9 involved the lung/pulmonary artery; 1 chest wall; 14 other vascular sites; 14 extravascular distant sites such as axilla, clavicle/neck/shoulder. Most were asymptomatic and detected when removal was requested. 7/38 reported symptoms such as pain, discomfort or dyspnoea. |
| Hindy 2020 | Case report + literature review. Asymptomatic right middle lobe pulmonary artery case, plus 11 previously published PubMed cases | Case: Issue detected at planned removal after 3 years when the implant was non-palpable. CXR showed an elongated right perihilar foreign body, CT angiography confirmed right middle lobe pulmonary artery migration, and the device was retrieved via right internal jugular venous access using an Ensnare loop. Review concluded that at least 21 pulmonary embolisation cases had been reported. |
| Simon 2020 | French surveillance study 906 reports of implant migration or removal complications; 27 pulmonary vascular migrations identified after duplicate exclusion | 19 specified as pulmonary artery migrations: left branch (9), right branch (4), unspecified (6. Discovery occurred at requested removal in 59%, after respiratory complaints in 24%, and because the implant was no longer palpable in 17%. Of 24 cases with management data, 15 were removed and 9 left in situ. Reported migration incidence estimated at 1.76/100,000 implants overall, with a 2017 peak of 3.17/100,000. |
| Clermidy 2022 | Tertiary referral cohort. 8 patients referred with pulmonary artery migration between 2015 and 2020 | Implants located in upper lobes (2) and lower lobes (6). Five patients had pulmonary symptoms, most commonly chest pain and dyspnoea. Endovascular retrieval was attempted in all 8 and succeeded in 3. In the 5 failures, angiography showed arterial thrombosis distal to the implant; all 5 then underwent successful open mini-thoracotomy under 5 cm, without serious post-operative complications. Two of the 3 successful endovascular retrievals had early diagnosis within 3 months. |
| Wali 2021 | Case report + literature review One surgically managed case plus comparison with prior literature | Case: Patient had return of irregular menstruation and a missing implant. Imaging showed a 4 cm linear opacity in a subsegmental branch of the left pulmonary artery. Mini-thoracotomy and arteriotomy failed to retrieve it, requiring segmentectomy. The implant was completely endothelialised within the arterial wall. They noted that most reported embolised implants were distal and technically difficult targets, and cited a high proportion in the left lower lobe. |
| Maybury 2024 | Case report + literature review Their own surgical case plus a compiled review of reported pulmonary vascular migrations | Case: Asymptomatic 22-year-old with a non-palpable implant at elective removal. Imaging showed migration to a distal left pulmonary artery branch; endovascular retrieval failed because the implant was encapsulated/adherent, and VATS left lower lobe basilar S7–9 segmentectomy was required. Compiled review: reported 55 prior cases 21 successful endovascular retrievals, 13 left in situ, 11 straight to VATS, 6 failed endovascular retrieval followed by successful VATS, 2 failed endovascular retrieval left in situ, and 3 unknown outcomes. |
| Kareem 2025 | Case report + literature review One very delayed case, with prior literature context | Case: Woman in her late 30s had a non-palpable implant 1 week after insertion but no investigation until years later. Imaging showed a subsegmental left lower lobe pulmonary arterial implant. Because she was asymptomatic, the implant appeared stable and was likely endothelialised after 6 years, conservative follow-up was chosen. The paper also notes that marketing-authority reports greatly exceed individually published cases. |
14. What should clinicians learn?
A missing implant should not be dismissed as “deep”, “difficult to feel”, or presumed expelled. Correct superficial insertion, immediate confirmation of palpability, patient education about self-palpation, and prompt localisation of non-palpable implants are central prevention and detection steps.
If a radiopaque implant cannot be found in the arm, the chest must be included in the search.
References
- Ismail H, Mansour D, Singh M. Migration of Implanon. J Fam Plann Reprod Health Care. 2006 Jul;32(3):157-9.
- Patel A, Shetty D, Hollings N, Dodds N. Contraceptive implant embolism into the pulmonary artery. Ann Thorac Surg. 2014 Apr;97(4):1452
- D’Journo XB, Vidal V, Agostini A. Intravascular pulmonary migration of a subdermal contraceptive implant. Ann Thorac Surg. 2015;99(5):1828
- O’ Brien A, O’Reilly MK, Sugrue G, Lawler L, Farrelly C. Subdermal Contraceptive Implant Embolism to a Pulmonary Artery. Ann Thorac Surg. 2015 Jun;99(6):2254-5
- Heudes PM, Laigle Querat V, Darnis E, Defrance C, Douane F, Frampas E. Migration of a contraceptive subcutaneous device into the pulmonary artery. Report of a case. Case Rep Womens Health. 2015 Sep 24;8:6-8.
- Kang S, Niak A, Gada N, Brinker A, Jones SC. Etonogestrel implant migration to the vasculature, chest wall, and distant body sites: cases from a pharmacovigilance database. Contraception. 2017 Dec;96(6):439-445.
- Gallon A, Fontarensky M, Chauffour C, Boyer L, Chabrot P. Looking for a lost subdermal contraceptive implant? Think about the pulmonary artery. Contraception. 2017 Feb;95(2):215-217
- Cerato A, Luyckx M, Ghaye B. Migration of implanon contraceptive implant into the pulmonary artery. Diagn Interv Imaging. 2019 Jan;100(1):59-60.
- Hindy JR, Souaid T, Larus CT, Glanville J, Aboujaoude R. Nexplanon migration into a subsegmental branch of the pulmonary artery: A case report and review of the literature. Medicine (Baltimore). 2020 Jan;99(4):e18881.
- Simon C, Maurier A, Gaboriau L, Vrignaud L, Dayani P, Vaillant T, Andrée Bos-Thompson M, Jonville-Bera AP. Incidence and characteristics of intravascular pulmonary migration of etonogestrel implants: A French nationwide study. Contraception. 2020 Sep;102(3):186-189.
- Shekarforoush M, Chapman S, Moriarty HK, Koukounaras J, Goh GS, Clements W. Implanon NXT embolisation into the pulmonary arterial tree. Aust J Gen Pract. 2020 Sep;49(9):585-586
- Wali A, Bilkhu R, Rizzo V, Bille A. Contraceptive implant migration to the lung. BJR Case Rep. 2021 May 12;7(4):20200216
- Clermidy H, Fabre D, Hugues JN, Alonso CG, Mitilian D, Mercier O, Brenot P, Charbonneau P, Fadel E. Management of Etonogestrel implant migration into the pulmonary artery. Contraception. 2022 Sep;113:62-67.
- Enabi J, Al-Ayyubi R, Amador P, Herrera A, Deepika D. Migration of a Contraceptive Subdermal Device Into the Lung. Cureus. 2023 Nov 2;15(11):e48179
- Maybury EK, Affrin ZC, Popa C, Fowler M, Laliberte BD, Clarke SC. Nexplanonectomy-the surgical removal of an embolized implanted contraceptive device: a case report and review of the literature. J Med Case Rep. 2024 May 2;18(1):234.
- Borg M, Swaminathan M, Cheuk J, Michael J, Walker G. Early endovascular retrieval of a migrated Implanon NXT from a branch of the right pulmonary artery. BMJ Case Rep. 2024 Aug 14;17(8):e261381.
- Kareem T, Frain D, Raza S, Watson NA. Subdermal contraceptive implant migration to pulmonary artery branch. BMJ Case Rep. 2025 Jan 30;18(1):e262771.
- Cadogan M. Exogenous Calcium Embolism. LITFL
- MIMS Australia. Implanon NXT CMI. Australian Commission on Safety and Quality in Health Care. Published in April 2025. Accessed on June 8, 2026.

CLINICAL CASES
Pulmonary Puzzler

MBBS, Curtin University. Junior doctor working at Sir Charles Gairdner Hospital. Interested in Emergency Medicine, education and baking.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
