
![]()
Frank J. Murphy
Francis John Murphy (1900 – 1972) was an American anaesthetist.
In 1940 Murphy became dissatisfied with the endotracheal tubes he was using and began to consider the characteristics of the ideal endotracheal tube and designing them. The materials he chose for composition are no longer used in modern ETT tubes but the Murphy Eye, an important safety feature, still is. This secondary hole allows another passage for oxygen flow if the distal end of the ETT becomes occluded.
Murphy is eponymously remembered for first describing the second hole on the end of the endotracheal tube (ETT), commonly referred to as the ‘Murphy eye‘.
Biography
- Born on March 11, 1900 in Oldham, South Dakota.
- 1925 – M.D., C.M. from McGill Medical School, Montreal.
- 1927 – Training in anaesthesia, Montreal General Hospital.
- 1930 – Chief of Anaesthesia at Harper Hospital, a position he held until 1941
- 1941 – Military service in World War II working within the Navy.
- 1945 – Chief of Anaesthesia at the Naval Hospital, Pearl Harbour.
- 1946-1956 Chief of Anaesthesiology, University of California Hospital in San Francisco
- 1970 – Retired to a ranch at Spirit lake, Idaho.
- Died in February 23, 1972 of a urological malignancy.
Medical Eponyms
Murphy Endotracheal Tube and the Murphy eye (1941)
The Murphy eye is a hole at the tip of the endotracheal tube to prevent tube obstruction if the beveled end of the tube is obstructed by mucus or sealed by contact with the tracheal wall. By the 1950’s it was present on most Magill endotracheal tubes, and the eponyms of ‘Murphy eye‘ or ‘Murphy tube‘ became standard.
Murphy determined that the ideal intratracheal catheter should possess certain characteristics which may be listed as follows:
- (a) Sufficient flexibility to accommodate itself to the pharynx and larynx.
- (b) Sufficient elasticity to prevent irritation to the parts through which it passes.
- (c) Sufficient body to resist the compression to which it would ordinarily be subjected when in use.
- (d) Resistance to kinking when bent at a moderately acute angle.
- (e) Ease of sterilization, (preferably by heat).
- (f) Durability in spite of repeated sterilizations.
- (g) Ease of insertion.
- (h) Adequate diameter of lumen in relation to outside diameter
- (i) Availability in a sufficient range of sizes.
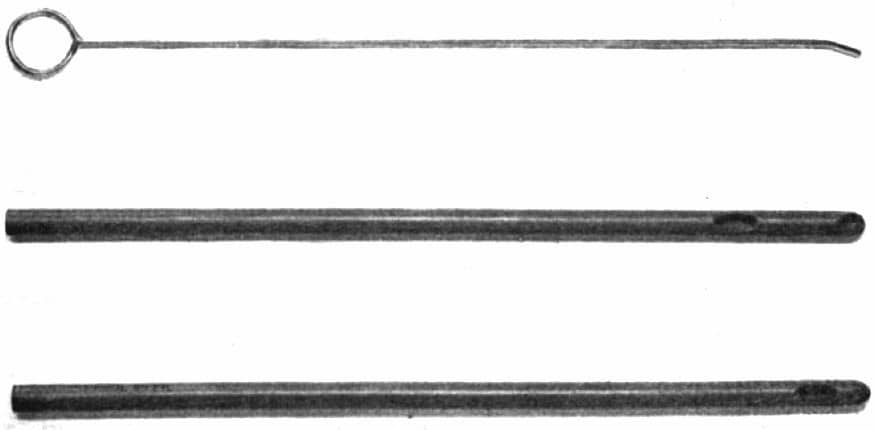
In addition to the eyes at the end of the tube, there are two other lateral eyes. Thus the total area of the openings in the end of the tube is much greater than the cross section of the lumen. This is of importance because should one or more of the eyes become obstructed with mucus, breathing is still not embarrassed…These catheters have been used by the author for several hundred cases, and have been found entirely satisfactory wherever the intratracheal method has been indicated.
Murphy 1941

Above, Murphy curved nasal tube with one eye, these were 31cm long with a whistle-tip ends. These were moulded and they retained their shape despite repeat sterilisation. Murphy believed the whistle-tip facilitated intubation, he thought the bevel of a Magill tube frequently caught on the vocal cords and caused kinking.
Major Publications
- Murphy FJ. Pre-anesthetic medication. Anesth Analg 1940; 19: 359–60
- Murphy FJ. Anesthesia in shock. Journal of the Michigan State Medical Society 1940; 39: 755–6
- Murphy FJ. Anesthesia and anoxemia in relation to the use of nitrous oxide. Surgery, Gynecology & Obstetrics 1940; 70: 741–3
- Murphy FJ. Two improved intratracheal catheters. Anesth Analges. 1941; 20(2): 102-105. [Murphy Eye]
Murphy FJ. The role of the anesthetist in relation to atelectasis. Harper Hospital Bulletin 1941; 1: 13–15 - Murphy FJ, Guadagni NP, DeBon F: Use of steroid anesthesia in surgery. JAMA 1955; 158: 1412–4
References
Biography
- Forestner JE. Frank Murphy, the Murphy Eye, and Mid-Century Anesthesia. Anesthesiology 2008; 109 A1361
- Forestner JE. Frank J. Murphy, M.D., C.M., 1900–1972: His Life, Career, and the Murphy Eye. Anesthesiology. 2010; 113(5): 1019-102
- Maltby R. Notable Names in Anaesthesia. The Choir Press; 203:151-153.
Eponymous terms
- Watersd RM, Rovenstine EA, Guedel AE. Endotracheal Anesthesia and Its Historical Development. Anesthesia and Analgesia. 1933; 12(5): 196-203
- Tamakawa S. Every endotracheal tube needs a Murphy eye! Can J Anaesth. 1999; 46(10): 998-9.
- McKennedy C. Murphy eye – Eponym A Day. Instagram
Eponym
the person behind the name

British doctor, working in Perth. Studied at Leeds University, graduated with an MBChB and BSc in Microbiology. Interests include netball and critical care.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |