
![]()
Funtabulously Frivolous Friday Five 344
Just when you thought your brain could unwind on a Friday, you realise that it would rather be challenged with some good old fashioned medical trivia FFFF, introducing the Funtabulously Frivolous Friday Five 344
Question 1
An Australian child, a British child, a New Zealand child and a Canadian child all walk into your emergency having swallowed their retrospective countries 2 dollar coins.
Who will walk out unscathed, and who will require an endoscopy?
Reveal the funtabulous answer
If anyone will escape a procedure it will be the Australian child but even they might require intervention.
Clue: These are the diameters of the coins
- Australian 20.5mm in diameter,
- New Zealand 26.5mm in diameter
- Canadian 28mm in diameter.
- British 28.4mm in diameter
Professor Nikolaos Salessiotis realised no one actually knew the diameter of the pylorus and what could feasibly pass. In 1972 he found 15 volunteers who in exchange for any meals they desired he would place a double-walled balloon on the end of a Levin tube and take a series of x-rays of the balloon inflated with lipiodol. The balloon was inflated to 2.5 and none passed after a regular meal and beverage. Again at 2.0cm and no action. Then at 1.9cm results started to occur, 4 volunteers could pass the balloon, 9 at 1.8cm and the final two at 1.7cm. Nikolaos concluded the upper limit for us to pass foreign bodies was 1.9cm.
Now, this becomes the origin of the 2cm threshold for foreign objects including the size of button batteries (i.e. even a 2cm button battery in the stomach will likely envoke an endoscopy) and coins requiring earlier x-ray follow up. Indeed this has been the case in practice as well. While I can not 100% say the Australian child won’t pass this coin, the others certainly do not stand a chance.
Reference:
- Pugh A, Schunk J, Ryan S. A 3-year-old boy with rapid obstructive symptoms secondary to coin ingestion and gastric impaction. J Am Coll Emerg Physicians Open. 2021 Jan 25;2(1):e12382.
- Salessiotis N. Measurement of the diameter of the pylorus in man. I. Experimental project for clinical application. Am J Surg. 1972 Sep;124(3):331-3.
- Tander B, Yazici M, Rizalar R, Ariturk E, Ayyildiz SH, Bernay F. Coin ingestion in children: which size is more risky? J Laparoendosc Adv Surg Tech A. 2009 Apr;19(2):241-3
Question 2
For many of us, the cold and flu season is back. The recent past has seen many advances in our armamentarium against viruses but the common cold still remains elusive.
What novel therapy did 4 German authors discover that could improve your nasal function to the same effect as a nasal decongestant?
Reveal the funtabulous answer

Eighteen couples (each 1 male and 1 female) enrolled in the study. resulting in 36 participants. For evaluation of subjective nasal breathing, a visual analogue scale (VAS) from 0 (no impairment) to 10 (no nasal breathing possible) was applied. For objective data, nasal resistance and flow were measured with a portable rhinometric device. The measurements were obtained at the participants’ homes by themselves.
Assessments of nasal function were performed at 5 specific points namely (1) before sexual activity (baseline), (2) immediately after orgasm, (3) 30 minutes, (4) 1, and (5) 3 hours after sexual climax.
The data were only obtained if both individuals experienced sexual orgasm. Same data were collected for the study participants on the following day after the application of nasal decongestant spray (0.1% xylometazoline; 1 application per side).
The data reported that nasal breathing improved up to 60 minutes after sexual intercourse and exactly to the same extent as a nasal decongestant.
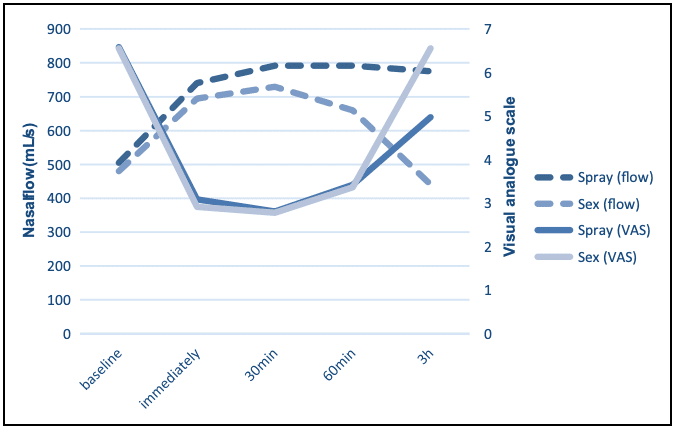
before and after interventions (sexual activity and application of nasal
decongestant spray). VAS indicates visual analogue scale. Bulut et al 2021
This paper didn’t just spike the interest of the FFFF judges but also the crew of the 2021 Ig Nobel prize. The paper won the medical section. For full details see the reference below.
Reference:
- Bulut OC, Oladokun D, Lippert BM, Hohenberger R. Can Sex Improve Nasal Function?-An Exploration of the Link Between Sex and Nasal Function. Ear Nose Throat J. 2021 Jan 4
- The 31st First Annual Ig Nobel Ceremony. 2021
Question 3
For over 70 years it has been known that hyperglycaemia can cause hyponatraemia.
Seldin and Tarail first proposed a correction factor of 2.8 mEq/L (or 2.8 mmol/L) of sodium for every 100 mg/dL (5.6 mmol) increase in glucose. This was based on the assumption that 100 mg/dL of glucose would behave osmotically as 2.8 meq of sodium. Katz later argued that the correction factor should be 1.6 mEq/L as the movement of water would cease before normal extracellular osmolality was restored.
The Katz formula is commonly used today. But who is closer to the truth, is it 2.8, 1.6 or somewhere in the middle?
Reveal the funtabulous answer
Somewhere in the middle – 2.4.
Surprisingly Seldin, Tarail and Katz were all just running hypothetical equations to predict what the correction factor would be. No one had actually studied it in humans. It wasn’t until Hillier et al in 1999 rendered 6 healthy subjects insulin-deficient with somatostatin and infused them with 20% dextrose that we had our first in-vivo study.

Hillier et al concluded that the correction factor of 1.6 meq/L Na per 100 mg/dL glucose was a considerable underestimation. By their calculations, 2.4 had a better overall estimate although they note at glucose levels >400 mg/dL (>22.2 mmol) the correction factor was closer to 4.
Let’s just be thankful we had MDCalc but when you see two correction results, which you will, this is the back story.
References
- Seldin DW, Tarail R. Effect of hypertonic solutions on metabolism and excretion of electrolytes. Am J Physiol. 1949 Oct;159(1):160-74
- Katz MA. Hyperglycemia-induced hyponatremia–calculation of expected serum sodium depression. N Engl J Med. 1973 Oct 18;289(16):843-4
- Hillier TA, Abbott RD, Barrett EJ. Hyponatremia: evaluating the correction factor for hyperglycemia. Am J Med. 1999 Apr;106(4):399-403
Question 4
Who invented the first battery operated laryngoscope?
Reveal the funtabulous answer
Henry Harrington Janeway (1873-1921)
Janeway was an American physician and pioneer for radiation therapy in the treatment of cancer.
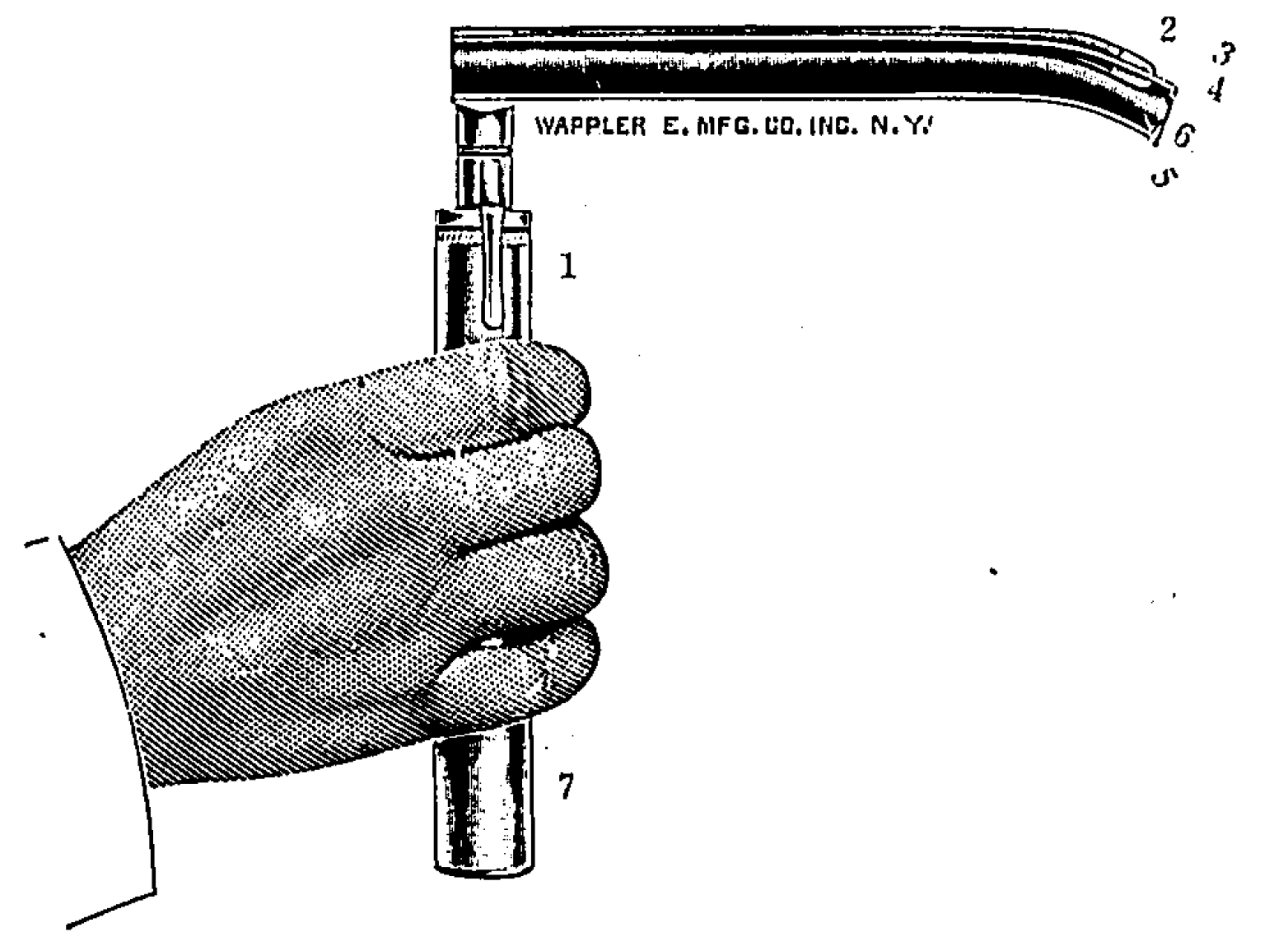
Janeway Laryngoscope (1913)
Janeway was the first anaesthetist to publish an article on direct laryngoscopy; prior articles about laryngoscopy were within the domain of surgeons. His landmark paper ‘intratracheal anaesthesia from the standpoint of the nose, throat and oral surgeon with a description of a new instrument for catheterising the trachea’ introduced the novel design of a battery powered laryngoscope, the first of its kind specifically designed for anaesthesia. Initial designs were complex and included a telescopic prism with eye piece to visualise the catheter and larynx. A central notch kept the catheter midline during placement
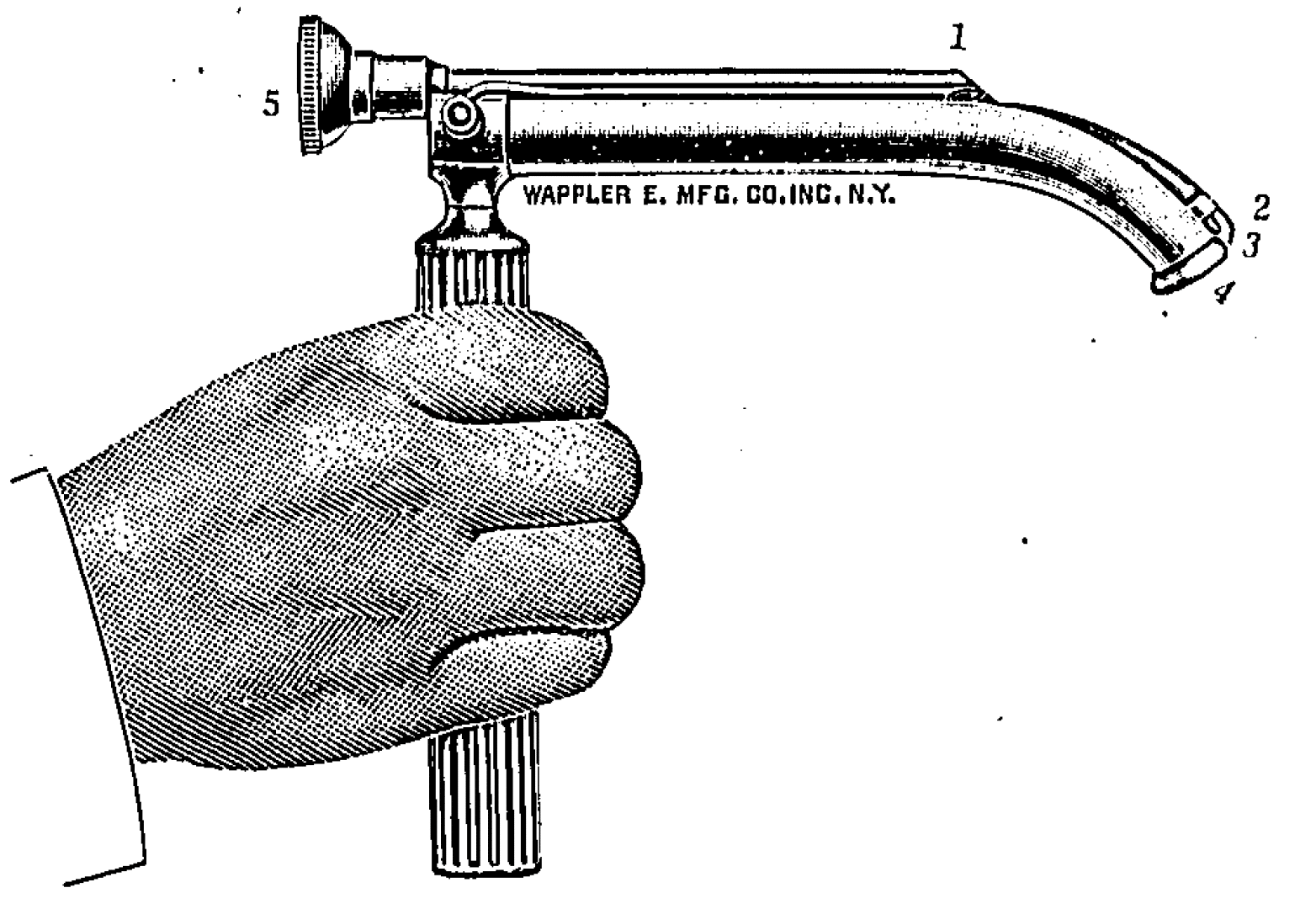
He later improved on this to include a distal light source with the battery incorporated within the handle of the laryngoscope itself and a blade that was shortened and curved at its distal end to facilitate delivery of the catheter through the vocal cords. Because catheter placement could now occur under direct vision, it obliviated the need for the complex prism mechanism.
Of his invention, he remarks:
…offers a very great advantage. It permits of easy catheterization of the larynx even when the patients’ pharyngeal reflexes are not completely abolished and without the necessity for the same degree of extension of the head. The omission of the telescope greatly simplifies the instrument
Laryngoscope. 1913
Whilst Janeway experienced much success with his invention in head and neck and thoracic procedures, his laryngoscope never gained widespread popularity
Question 5
Do you remember those 2-3 weeks of rheumatology at medical school? There was a joint examination, in fact there was a score for assessing hypermobile joints. Maybe you remember the name, the Beighton Score.
What is the Beighton Score, and who was it named after?
Reveal the funtabulous answer
Okay, so no points for saying, Dr Beighton.
Of course, Peter Beighton was involved, but behind every great man, is a great woman and it was his wife Greta Beighton, who developed the scoring system. Dr Beighton has actively sought to correct any connotation that she was not involved in recent years, stating he was initially concerned about nepotism.
History of the Beighton Score
1964 – A standardised method for the clinical assessment of joints at the following anatomical sites was proposed by Carter and Wilkinson. A five-point score was proposed in order to provide a numerical perspective of the degree of joint hypermobility:
- Passive dorsiflexion of the little fingers beyond 90 degrees.
- Passive apposition of the thumb to the flexor aspect of the forearm.
- Hyperextension of the elbows beyond 10 degrees.
- Hyperextension of the knee beyond 10 degrees.
- Forward flexion of the trunk with knees fully extended so that the palms of the hands rest flat on the floor.
1967 – Kirk, Ansell and Bywaters introduced he term “Hypermobility Syndrome”.
1967-1968 Peter Beighton undertook a survey of 100 persons and families with the Ehlers-Danlos Syndrome at St Thomas’ Hospital, London. Affected families were seen in their homes throughout southern England and PB was accompanied and assisted on this Doctoral project by a nursing sister, Greta Winch. The patients’ join movements were assessed using the method and the 5-point scale proposed by Carter and Wilkinson, 1964.
1970 – Peter and Greta Beighton (now married) travelled to South Africa to undertake an epidemiological investigation of bone and joint disorders, based at the University of the Witwatersrand. An initial recognisance was undertaken in a semi-nomadic Bushmen community in the Kalahari Desert. Project plans were discussed while sitting around the camp fire. Greta had a flash of insight and suggested that although the limbs and digital joins were paired, they were not necessarily symmetrical and that a 9-point score would be appropriate.
1971 – Greta’s 9-point score was successfully used in a formal epidemiological survey of 1081 persons in a Tswana community in the Transvaal, South Africa. Details of the project were presented by Peter Beighton at a meeting of the Herberden Society in London in Nov 1972. The results were published under the names Beighton, Solomon and Soskolne in 1973
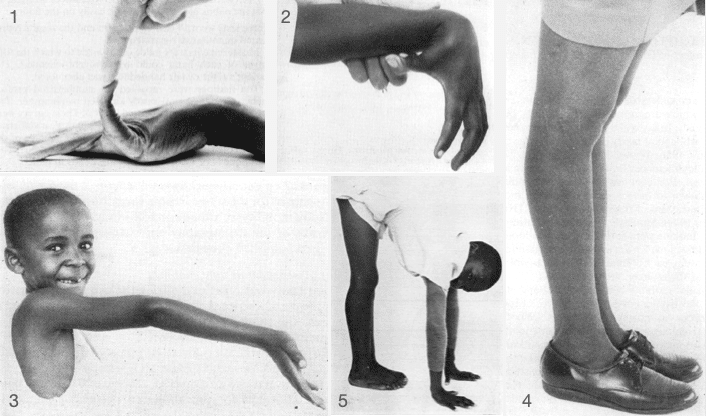
- Fig 1: Hyperextension of the fifth finger [In this particular illustration, the extension angle does not reach the required 90o
- Fig. 2 Apposition of the thumb to the ventral aspect of the forearm
- Fig 3. Hyperextension of the elbow joint beyond 10o
- Fig 4. Hyperextension of the knee joint beyond 10o
- Fig 5. Placing the palms of the hands flat on the floor while maintaining the knees in full extension
The method of assessing joint mobility by means of a score based upon the range of movements of certain joints has proved its value in previous investigations. Although the great majority of normal adults score values of 0, 1, or 2 on the mobility scale, individuals with inherited hypermobility syndromes achieve scores at the top end of the scale (Beighton and Horan, 1969). It is therefore reasonable to conclude that the scale is valid for the measurement of joint mobility.
The results which were obtained demonstrate that the range of movements decreases with age, falling rapidly during childhood, and more slowly throughout adult life. However, at any age, females are consistently more hypermobile than males.
Beighton et al 1973
2020 – Peter Beighton comments:
Following her initial suggestion in 1971 concerning the 9-point score, Greta Beighton retained her involvement in the elucidation and publication of research material in the broad field of hypermobility for almost 50 years.
During this period, she typed and compiled ten books and more than 400 articles in medical journals. As a matter of principle, rightly or wrongly, her name was deliberately withheld from the deserved co-authorship in order to avoid any suggestion of nepotism. This article is essentially a posthumous attempt to ensure the eponymous recognition that she richly deserves.
Peter Beighton 2020, personal communication
…and Finally
- Nature does Open Access. Dr. Glaucomflecken

FFFF
Funtabulously Frivolous Friday Five
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |