
![]()
Gaston Labat

Louis Gaston Labat (1876–1934) was a Seychellois-born, French-trained physician and pioneer of regional anaesthesia
After early life in the Seychelles and Mauritius, Labat studied medicine in Montpellier and Paris, where he worked with Victor Pauchet and became immersed in the French school of regional anaesthesia. In 1920, after Charles H. Mayo observed his regional anaesthetic work in Paris, Labat was invited to the Mayo Clinic to teach regional anaesthesia and prepare an English-language textbook for American practice.
Labat’s major contribution was the standardisation and dissemination of regional anaesthesia in North America. His textbook Regional Anesthesia (1922) described surface anatomy, needle technique, block indications, and clinical application with great clarity. He is remembered for the Labat approach to sciatic nerve block, the classic posterior landmark technique using the posterior superior iliac spine and greater trochanter to locate the injection point.
Labat is associated with a purpose-built nickel spinal puncture needle and a portable regional anaesthesia outfit. His spinal needle was designed to be robust, sterile, and technically reliable It was medium gauge, short bevelled, and fitted with a matching stylet. The Labat outfit placed the needle within a complete sterilizable system of syringes, needles, and instruments for regional, spinal, caudal, and epidural block. Labat founded the American Society of Regional Anesthesia in 1923 and remains a central figure in the transition of regional anaesthesia from surgeon-performed technique to organised anaesthetic discipline.
Biographical Timeline
- Born on December 11, 1876 Victoria, Mahé, Seychelles to French parents Siméon Labat and Marie Labat. His birth was registered in January 1877, which has led to occasional confusion about the year of birth.
- 1883 – Following the death of his father in a shipwreck, Labat moved with his mother and sisters to Mauritius, where he spent much of his childhood and early education.
- 1894 – Graduated with honours from the Royal College of Mauritius, with certificates in English, French, mathematics, mechanics, physics, and chemistry.
- 1890s–1900s – Worked in his brother-in-law’s pharmacy in Mauritius, gaining practical experience with chemistry, medicinal compounds, and patient care.
- 1913 – Moved to France and completed baccalauréat studies in natural sciences, physics, and chemistry before entering medical training.
- 1914–1916 – Medical student at the University of Montpellier; served as an intern in surgery at l’Hôpital Général de Montpellier.
- 1916 – Transferred to the University of Paris to continue medical studies.
- 1917–1919 – Extern in surgery at Hôpital Pitié, Paris.
- 1918–1920 – Worked with French surgeon Victor Pauchet (1869-1936) assisting with regional anaesthesia techniques.
- 1920 – Received his medical degree from the University of Paris. Co-authored the third edition of Pauchet and Sourdat’s L’Anesthésie Régionale. Recruited to the Mayo Clinic after Charles H. Mayo observed Labat’s regional anaesthetic work in Paris. Served as special lecturer and clinical demonstrator in regional anaesthesia at the Mayo Clinic.
- 1921 – Left the Mayo Clinic under somewhat unclear personal and institutional circumstances and moved to New York City.
- 1922 – Published Regional Anesthesia: Its Technic and Clinical Application. Obtained United States medical licence and established practice in New York City; later served at New York University Medical College and Bellevue Hospital.
- 1923 – Founded the American Society of Regional Anesthesia and served as its first president. The original society later merged with the American Society of Anesthetists in 1941; the modern ASRA was re-established in 1975.
- 1924 – Developed teaching courses in regional anaesthesia at Bellevue Hospital and New York University, and established a private block clinic in New York City for chronic pain management.
- 1928 – Published the second edition of Regional Anesthesia.
- Died on October 1, 1934 in New York from postoperative complications following a cholecystectomy
- At the time of his death, Labat was preparing a third edition of Regional Anesthesia and apparently another manuscript on the therapeutic aspects of nerve blocking. The third edition was not published until 1967, edited by John Adriani
Key Medical Contributions
Regional anaesthesia in America
Labat’s major contribution was the introduction and standardisation of European regional anaesthesia techniques in the United States. Trained in Paris with Victor Pauchet, he arrived at the Mayo Clinic in 1920 at the invitation of Charles H. Mayo, who had seen his regional anaesthetic work in France. At Mayo, Labat taught regional anaesthesia through lectures, demonstrations, and clinical practice, helping shift nerve block from a surgeon’s occasional technique toward a reproducible anaesthetic discipline.
His influence was especially important because regional anaesthesia was still unfamiliar to many American surgeons and anaesthetists. Labat emphasised anatomical precision, appropriate block selection, asepsis, dose control, patient preparation, and the practical steps needed to make peripheral nerve block safe and repeatable.
Labat’s textbook, Regional anesthesia; its technic and clinical application, was first published in 1922, and became one of the foundational English-language works on regional anaesthesia. The book drew on his work with Pauchet, his Mayo Clinic demonstrations, and detailed practical illustrations to describe percutaneous nerve blocks, field blocks, spinal anaesthesia, and clinical applications across surgery.
Medical Eponyms
Labat approach to sciatic nerve block
Labat approach: classic posterior sciatic nerve block using the posterior superior iliac spine, greater trochanter, and a perpendicular from the midpoint of the iliotrochanteric line to identify the puncture site.
In his 1922 textbook, Labat described blocking the great sciatic nerve with the patient in a modified Sims position, lying on the side opposite the limb to be anaesthetised. The thigh was flexed on the pelvis and the leg flexed on the thigh to bring the posterior gluteal landmarks into view.
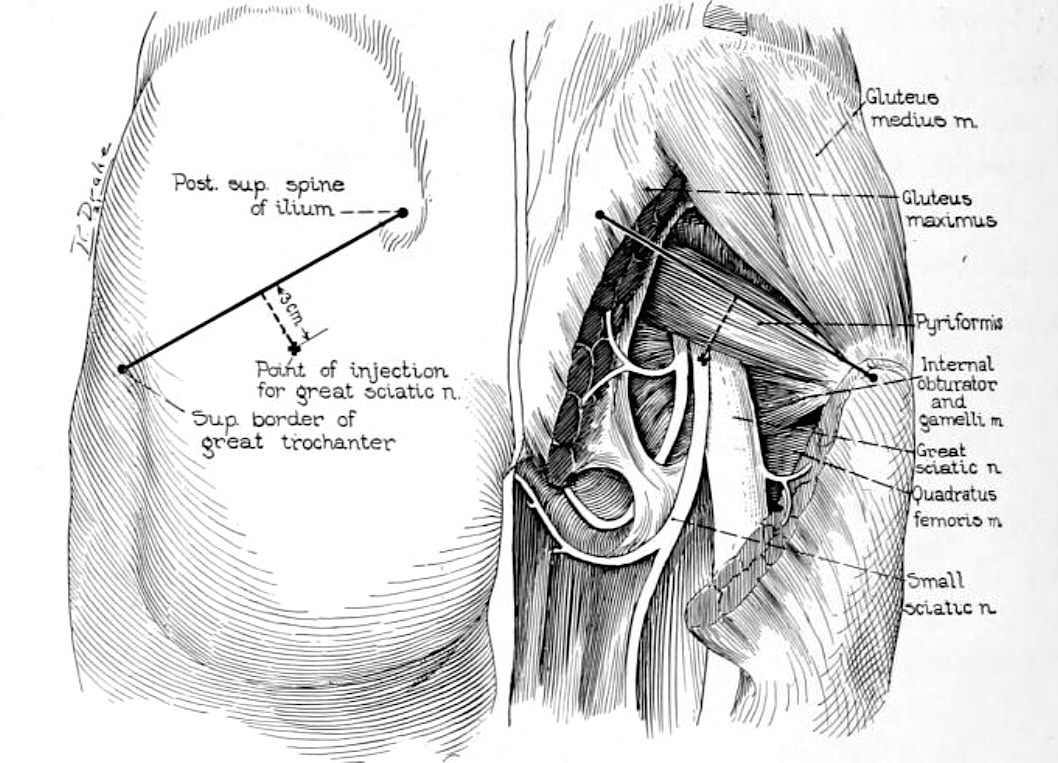
Labat used two landmarks, the posterior superior iliac spine and the upper extremity of the greater trochanter. A line was drawn between these points, then bisected. From the midpoint, a perpendicular line was drawn downward and inward and the puncture point placed approximately 3 cm along this perpendicular. A long needle was advanced perpendicular to the skin until paraesthesia was elicited or bone was contacted, then withdrawn slightly and redirected as required.
The technique became one of the enduring landmark-based approaches to lower-limb regional anaesthesia. The Labat approach highlights surface anatomy, geometric reproducibility, controlled needle placement, and clear clinical indications. The original figures are useful to demonstrate both the patient position and the relationship between the surface geometry and the deep gluteal anatomy.
Figure 1: Patient positioned almost in Sims’ position, lying on the opposite side with the hip flexed. The posterior superior iliac spine and superior border of the greater trochanter define the surface landmarks for the injection point.
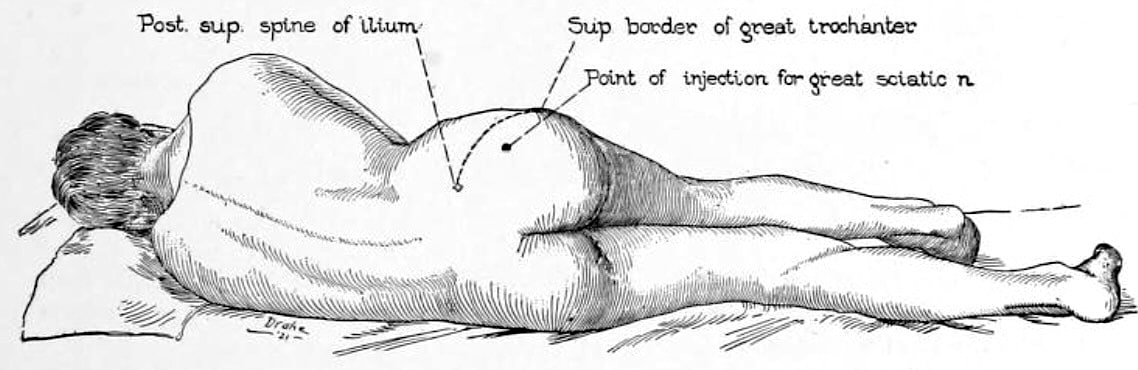
Figure 2: The injection point is constructed from the line between the posterior superior iliac spine and greater trochanter, with a perpendicular drawn from its midpoint. Labat related these landmarks to the great sciatic nerve, small sciatic nerve, piriformis, and short external rotators.
Labat spinal anaesthesia
Labat’s contribution to spinal anaesthesia was part of his broader effort to standardise regional anaesthetic practice. In his 1921 paper, “Latest achievements of the art of local, regional and spinal anesthesia,” he described spinal anaesthesia as a controlled technical procedure requiring appropriate drug choice, careful handling of cerebrospinal fluid, slow injection, patient preparation, and a proper anaesthetic outfit.
At the Mayo Clinic, Labat reported more than 100 spinal anaesthetics using novocain dissolved in the patient’s own cerebrospinal fluid. His emphasis was not simply on spinal puncture, but on making spinal anaesthesia reproducible, sterile, and predictable.
His preferred drug was novocain, which he considered the anaesthetic of choice for both regional and spinal anaesthesia. For spinal use, he advised pure sterile novocain dissolved in the patient’s CSF, at 0.01 g per 15 lb body weight, injected very slowly. He specifically avoided adrenaline in spinal anaesthesia, arguing that its vascular action was “of no avail in the spine.”
Labat spinal puncture needle
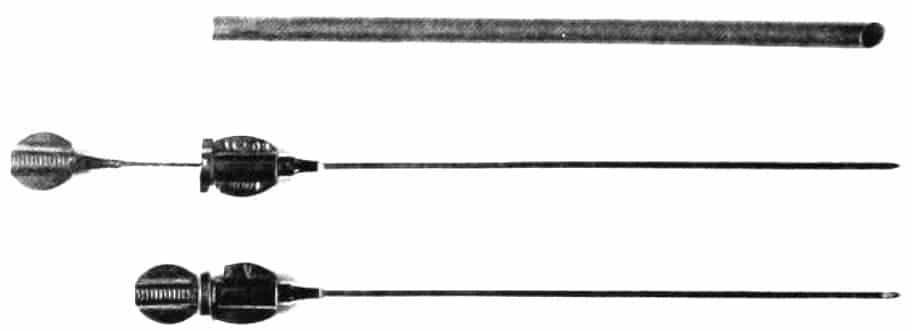
In his 1922 textbook, Labat described the features of an ideal spinal puncture needle. It should be of medium gauge (approximately 1.1 mm) to avoid excessively rapid CSF flow, limit injection speed, and leave only a small dural wound. It should be of medium length (approximately 80 mm) long enough for obese patients but short enough to allow stable hand support on the patient’s back.
Labat emphasised use of a short bevel, no more than 1.5 mm. He argued that a long bevel might remain partly outside the subarachnoid space, whereas a short bevel allowed the entire opening to pass through the dura without advancing the point unnecessarily toward the cord or cauda equina.
The needle also required a sharp point, controlled rigidity and flexibility, and a matching stylet ground flush with the bevel. Labat preferred nickel because steel rusted and could break, while platinum was too soft and bent easily. The stylet was secured by a hub pin-lock.
Labat therefore adopted a nickel spinal puncture needle because it was effectively “unbreakable” and reduced technical risk during spinal, caudal, or epidural block.
Labat regional anaesthesia outfit
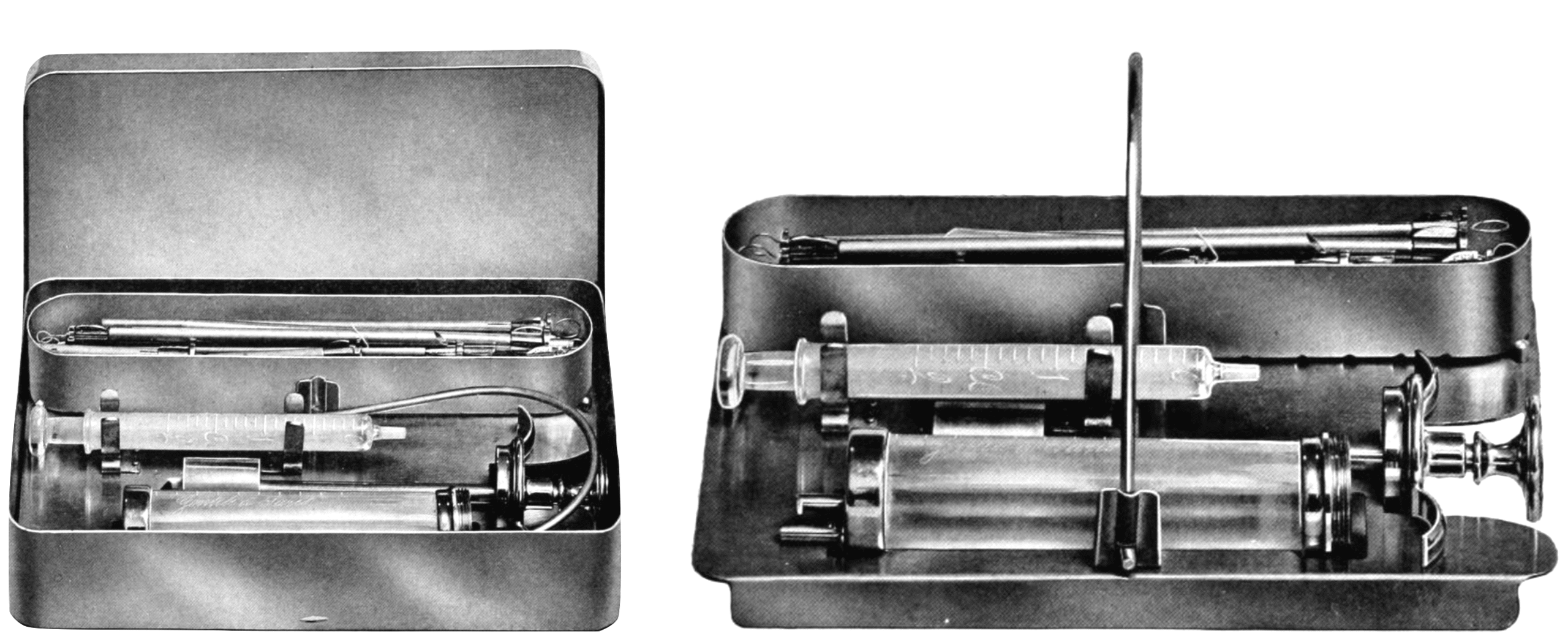
Labat placed the spinal needle within a system of sterile, portable regional anaesthesia equipment. His Labat outfit was a compact nickel-plated metallic case containing the syringes, needles, and instruments required for regional and spinal anaesthesia. The case and tray could be sterilised by boiling, dry heat, steam, or direct heating where no formal sterilizer was available.
The Labat Regional Anesthesia Outfit, manufactured by the Anglo-French Drug Company of New York, containing a syringe and needles specifically designed for regional anaesthesia. Labat emphasised that this was especially useful in hospitals, where several sterile outfits could be kept ready for emergency use.
Major Publications
- Labat G. Contribution à l’ʹetude de l’anesthʹesie paravertébrale en chirurgie gastrique et intestinale. 1920
- Pauchet V, Surdat P, Labat G. L’anesthésie régionale. Troisième édition refondue. 1921
- Labat GL. Latest achievements of the art of local, regional and spinal anesthesia. Ann Surg. 1921 Dec;74(6):673-83
- Labat G. Regional anesthesia; its technic and clinical application. 1922
- Labat G. Regional Anesthesia for Orthopedic Operations Upon the Spinal Column. Current Researches in Anesthesia & Analgesia 1928; 7(1): 38-44
- Labat G, Greene MB. Contribution to the modern method of diagnosis and treatment of the so-called sciatic neuralgias: Case reports. The American Journal of Surgery, 1931; 11(3): 435–450.
References
Biography
- Brown DL, Winnie AP. Biography of Louis Gaston Labat, M.D. Regional Anesthesia 1992; 17: 249-262.
Eponymous terms
- Bacon DR, Lema MJ. Gaston Labat and the American Board of Anesthesiology. Reg Anesth. 1993 Jan-Feb;18(1):64.
- Bacon DR. Gaston Labat, John Lundy, Emery Rovenstine, and the Mayo Clinic: the spread of regional anesthesia in America between the World Wars. J Clin Anesth. 2002 Jun;14(4):315-20.
- Côté AV, Vachon CA, Horlocker TT, Bacon DR. From Victor Pauchet to Gaston Labat: the transformation of regional anesthesia from a surgeon’s practice to the physician anesthesiologist. Anesth Analg. 2003 Apr;96(4):1193-1200.
- Finucane BT. Gaston Labat Lecture 2003: Labat’s legend–are we doing it justice? Reg Anesth Pain Med. 2003 Nov-Dec;28(6):540-6
- Pulido JN, Bacon DR, Rettke SR. Gaston Labat and John Lundy: friends and pioneer regional anesthesiologists sharing a Mayo clinic connection. Reg Anesth Pain Med. 2004 Sep-Oct;29(5):489-93.
- Vachon CA, Bacon DR, Rose SH. Gaston Labat’s Regional Anesthesia: the missing years. Anesth Analg. 2008 Oct;107(4):1371-5.
- Orkaby A, Desai S. Gaston Labat, the Mayo Clinic, and the Introduction of Regional Anesthesia to the United States. European Journal for the History of Medicine and Health, 2024; 81(1): 45-73.
- Labat Spinal Outfit. Wood Library Museum
- Gaston Labat Award. ASRA and Pain Medicine
- Harms R, Cadogan M. History of Spinal Needles. LITFL
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |