
![]()
George Pitkin
George Philo Pitkin (1885-1943) was an American surgeon, inventor, and pioneer of controllable spinal anaesthesia
Pitkin was a regional anaesthesia advocate based in Bergenfield and Teaneck, New Jersey. He served as chief surgeon at Holy Name Hospital and became one of the early twentieth-century American proponents of spinal and conduction anaesthesia. Pitkin is associated with controllable spinal anaesthesia, Spinocain, the Pitkin spinal needle, Pitkin San-a-lok syringe, and the Pitkin tiltometer.
Pitkin’s enduring contribution was not a single device, but a complete system of spinal anaesthesia. He sought to control the height, duration, intensity, and cardiovascular effect of spinal blockade through anaesthetic solution, patient positioning, needle design, and controlled injection.
Biographical Timeline
- Born on March 25, 1885 at Schroon Lake, Essex County, New York son of Philo H. Pitkin and Eliza Persons Pitkin
- 1908 – Graduated MD, Albany Medical College.
- 1910 – Established medical practice in Bergenfield, New Jersey
- 1925 – Instrumental in the founding of Holy Name Hospital, Teaneck, New Jersey; served as chief surgeon.
- 1927 – Published work on controllable spinal anaesthesia, developing Spinocain, the Pitkin spinal needle, and the Pitkin San-a-lok syringe as part of his regional anaesthesia system.
- 1929 – Presented “Spinocain: the controllable spinal anaesthetic” at the British Medical Association meeting, Manchester. Introduced the Pitkin tiltometer to measure Trendelenburg positioning during spinal anaesthesia.
- 1930 – Married Dr Winifred Mercer of England.
- 1941–1943 – Worked on his major regional anaesthesia textbook, Conduction Anesthesia, with assistance from his wife Winifred Mercer Pitkin and medical illustrator J. Eastman Sheehan. The work was incomplete at his death.
- Died on September 3, 1943 at Holy Name Hospital, Teaneck, New Jersey, after acute appendicitis complicated by peritonitis and pneumococcal bronchopneumonia.
Medical Eponyms
Controllable spinal anaesthesia
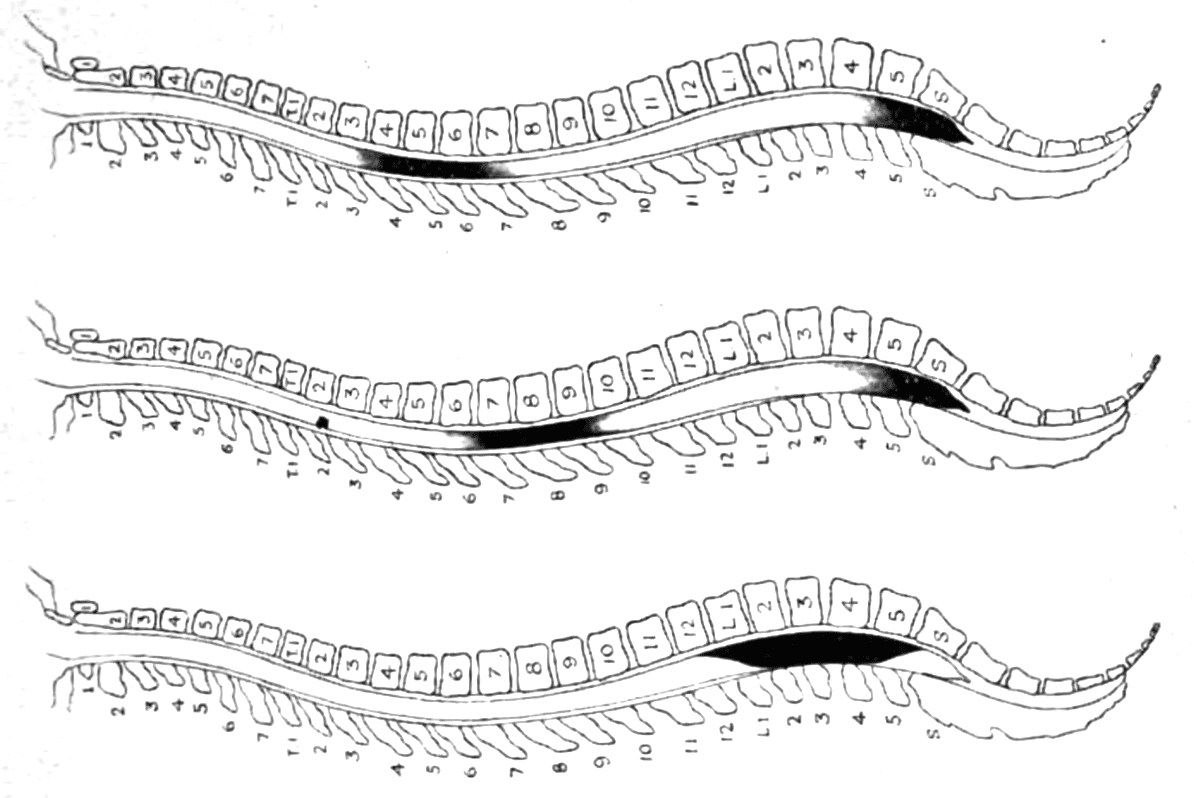
Pitkin’s central anaesthetic concept was “controllable spinal anaesthesia”. An attempt to make spinal anaesthesia predictable in height, duration, intensity, and cardiovascular effect. He argued that the major dangers of spinal anaesthesia came from uncontrolled cephalad diffusion of local anaesthetic in the CSF, producing hypotension, respiratory compromise, nausea, vomiting and collapse.
His solution combined several elements including a viscous hypobaric anaesthetic solution, controlled patient positioning, barbotage, vasopressor support, and careful attention to the volume and spread of spinal anaesthetic.
1927 – Pitkin developed his technique of controllable spinal anaesthesia using Spinocain, patient positioning, and barbotage. He presented the concept to the British Medical Association as “Spinocain: the controllable spinal anaesthetic.” in 1929
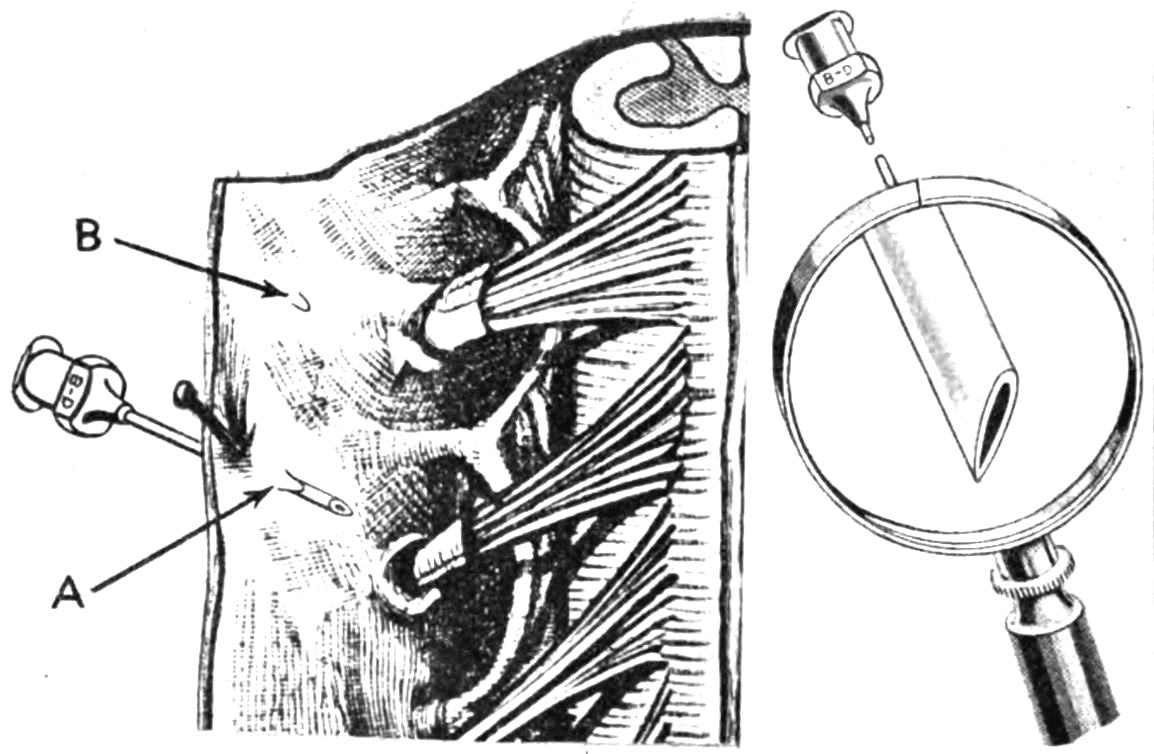
Pitkin spinal needle
The Pitkin spinal needle was a 20–22G rustless steel spinal needle with a short bevel ground to approximately 45°. Some versions had a collar to mark depth of insertion. Pitkin designed it to reduce CSF leakage after dural puncture.
The theoretical basis was the so-called “trapdoor” theory. Pitkin believed the short blunted bevel would create a dural flap that would close after withdrawal, limiting CSF escape. This theory was later challenged, but the design remains historically important because it recognised that needle tip geometry influenced the dural defect and post-dural puncture headache.
Pitkin’s Solution – Spinocain
Spinocain(e) was Pitkin’s proprietary spinal controllable spinal anesthetic agent. At the time the major objections to spinal anaesthesia included variable spread, short duration, hypotension, nausea, vomiting, and post-anaesthetic disturbance.
Pitkin designed Spinocain to provide a more manageable, targeted numbing effect without significant side-effects. His Solution combined
- Novocain (procaine) as the active anaesthetic agent. Considered the least toxic of the contemporary options
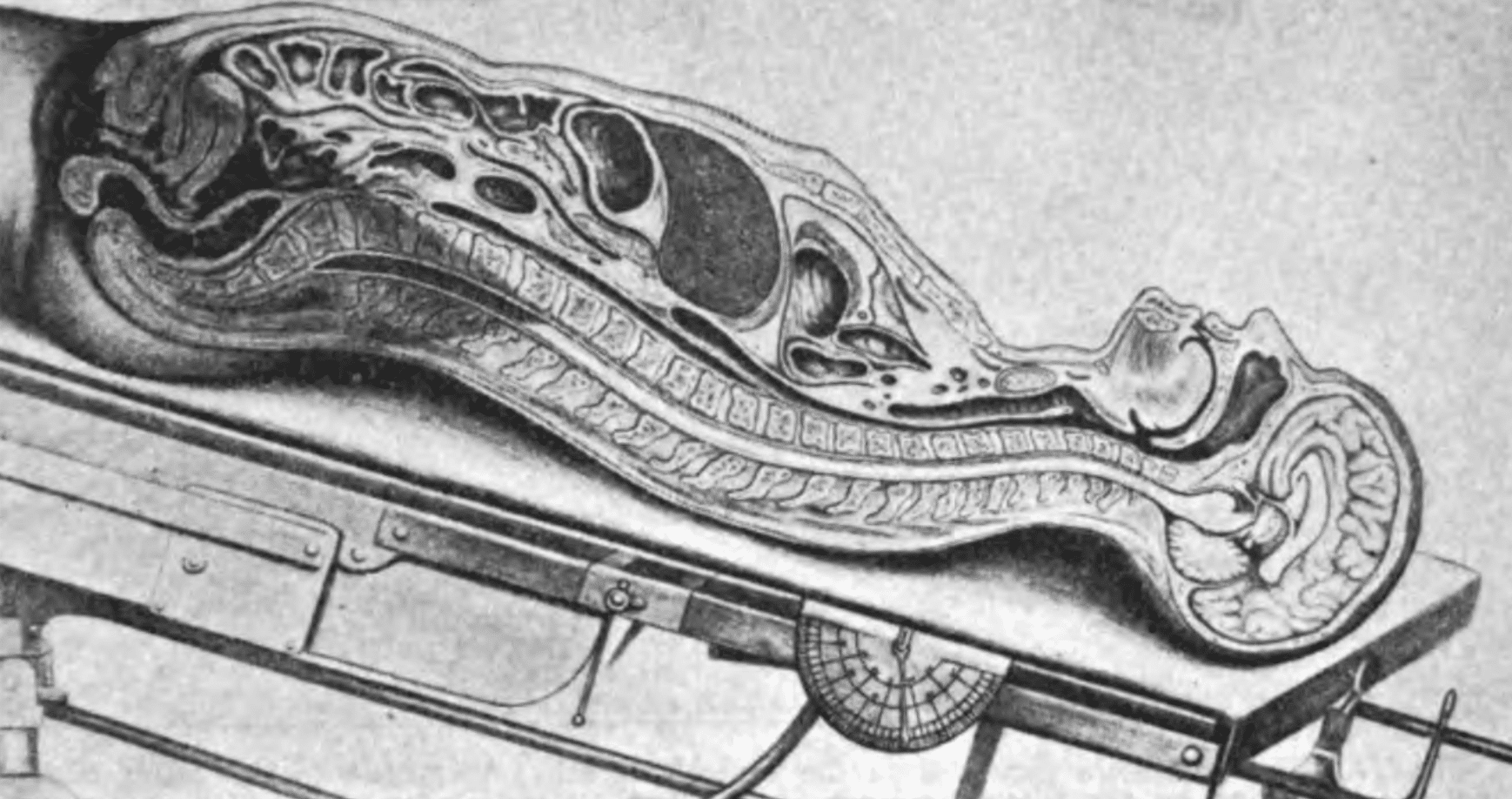
- Ethyl Alcohol as a buoyancy agent. This made the solution hypobaric (lighter than spinal fluid) and able to float like an air bubble, allowing the doctor to move the numbness by tilting the patient’s table
- Gliadin (starch paste) as a thickening agent. Increased viscosity reduced the rate of Novocain mixing with the spinal fluid
- Strychnine as a vasomotor constrictor and reduce risk of anaesthetic induced hypotension
Pitkin tiltometer
The Pitkin tiltometer was a device used to measure the angle of the operating table during spinal anaesthesia, particularly in the Trendelenburg position. Pitkin believed that patient position was central to controlling the spread of spinal anaesthetic.
Pitkin introduced the tiltometer in 1929 to accurately gauge table tilt when applying his controllable spinal anaesthesia technique.
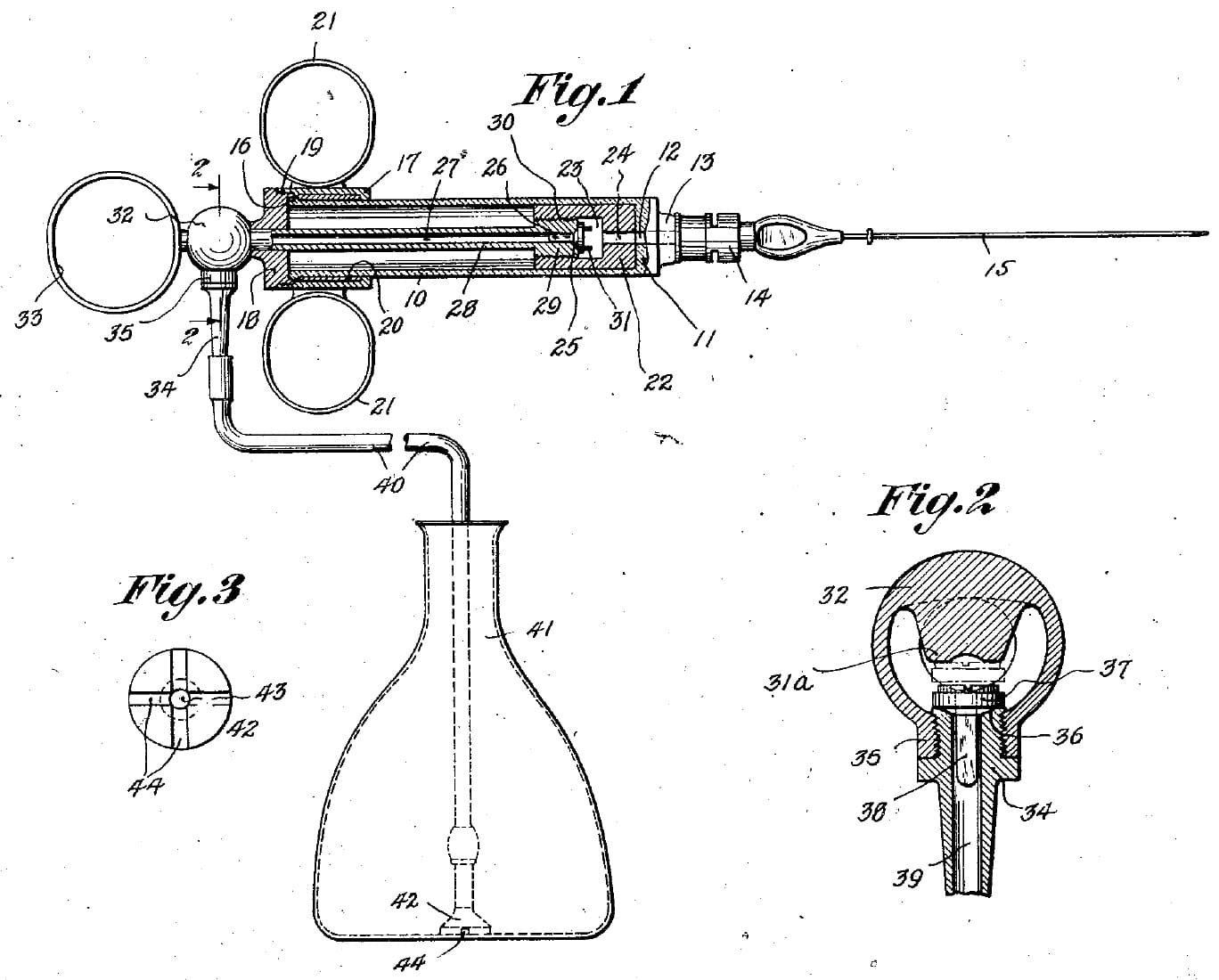
Pitkin syringe
The Pitkin syringe was a self-filling continuous-flow syringe designed for local and spinal anaesthesia. It allowed anaesthetic solution to be introduced through the piston and piston-stem, with backflow prevented by a valve, and incorporated a Luer-lock connection to prevent leakage or needle disconnection.
The syringe could be refilled through tubing without disconnecting the syringe or reinserting the needle multiple times, describing it as a step toward later continuous spinal anaesthesia.
Major Publications
- Pitkin GP. Luminous thermometer. US Patent US1338524A 1919
- Pitkin GP. Controllable spinal anesthesia. Journal of the Medical Society of New Jersey 1927; 24: 425–438.
- Pitkin GP. A safe and effectual anesthesia for thyroidectomies. Journal of the Medical Society of New Jersey 1927; 24: 603-611.
- Pitkin GP. Local-anesthetic syringe. US Patent US1681744A 1928
- Pitkin GP. Controllable spinal anesthesia. Am J Surg 1928; 5(6): 537-553
- Pitkin GP. Controllable Spinal Anesthesia with Spinocain. Anesthesia & Analgesia 1929; 8: 78-90
- Pitkin GP. Spinocain: The Controllable spinal anaesthetic. Br Med J. 1929 Aug 3;2(3578):183-187
- Pitkin GP. Spinal anesthesia in obstetrics and gynecology. American Journal of Obstetrics and Gynecology 1929; 18(2): 165-171.
- Pitkin GP. Conduction anesthesia for minor surgery. Am J Surg 1930; 8(2): 239-264
- Pitkin GP. A new treatment of peptic ulcer. Am J Surg 1931; 12(3): 466-478
- Pitkin GP. Prolonged local or block anesthesia with regulated cell reception. Anesthesia & Analgesia 1942; 21: 1-12 and 21(2): 83-95
- Pitkin GP. Conduction anesthesia. 1946 [2e 1953]
References
Biography
- Rosenberg H, Axelrod JK. Two surgeons who popularized spinal anesthesia. Reg Anesth Pain Med. 2001 May-Jun;26(3):278-82
Eponymous terms
- Pitkin Syringe. Wood Library Museum
- Pitkin Tiltometer. Wood Library Museum
- Harms R, Cadogan M. History of Spinal Needles. LITFL
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
