
![]()
Giovanni Battista Morgagni

Giovanni Battista Morgagni (1682-1771) was an Italian physician, anatomist and pathologist.
Morgagni is widely regarded as the father of modern anatomical pathology. Born in Forlì, Italy, he trained under Antonio Maria Valsalva at Bologna and later became professor of anatomy at Padua, where he transformed the study of disease by correlating clinical histories with autopsy findings. His monumental De sedibus et causis morborum per anatomen indagatis (1761) compiled more than 700 detailed case histories with post-mortem examinations, setting the template for clinico-pathological correlation.
Morgagni’s work spanned a remarkable range of medicine. He gave one of the earliest descriptions of what is now called Stokes–Adams syndrome, linking epilepsy-like attacks with profound bradycardia. His accounts of intestinal ulceration, strictures, fistulae, and abscesses in patients with chronic wasting illness have been retrospectively recognized as among the first descriptions of Crohn’s disease. In ophthalmology, he noted punctate cortical opacities in the lens, later termed Morgagni’s cataract. His attention to thoracic pathology, including aneurysms and cardiac enlargement, foreshadowed cardiovascular medicine.
Morgagni’s influence extended beyond his own discoveries. By insisting on anatomical proof for clinical claims, he established a method of reasoning that reshaped eighteenth-century medicine and laid the foundation for Virchow’s cellular pathology a century later. Today, he is remembered by eponyms including Morgagni’s hernia and the Foramen of Morgagni
Biographical Timeline
- 1682 – Born February 25 in Forlì, Papal States.
- 1698 – Entered the University of Bologna, studying medicine, philosophy, and natural sciences.
- 1701 – Received doctorate in philosophy and medicine at Bologna at age 19.
- 1701–1706 – Assistant to Antonio Maria Valsalva (1666–1723), contributing to anatomical dissections and publications.
- 1706 – Published Adversaria anatomica prima (first of six volumes, 1706–1719), establishing his reputation as an anatomist.
- 1712 – Appointed professor of theoretical medicine at the University of Padua.
- 1715 – Published further Adversaria anatomica volumes, including important observations on glands and vessels.
- 1715 – Married Paola Vergieri; the couple eventually had 15 children.
- 1717 – Succeeded Bernardino Ramazzini (1633–1714) as chair of medicine at Padua.
- 1720s–1750s – Continued to publish on anatomy, pathology, and clinical correlations; gained reputation across Europe.
- 1761 – Published De Sedibus et Causis Morborum per Anatomen Indagatis his landmark five-volume work correlating clinical symptoms with post-mortem findings in over 700 cases
- 1769 – Elevated to senator of Padua by the Venetian Republic in recognition of his scholarly contributions.
- 1771 – Died December 6 in Padua, aged 89.
Medical Eponyms
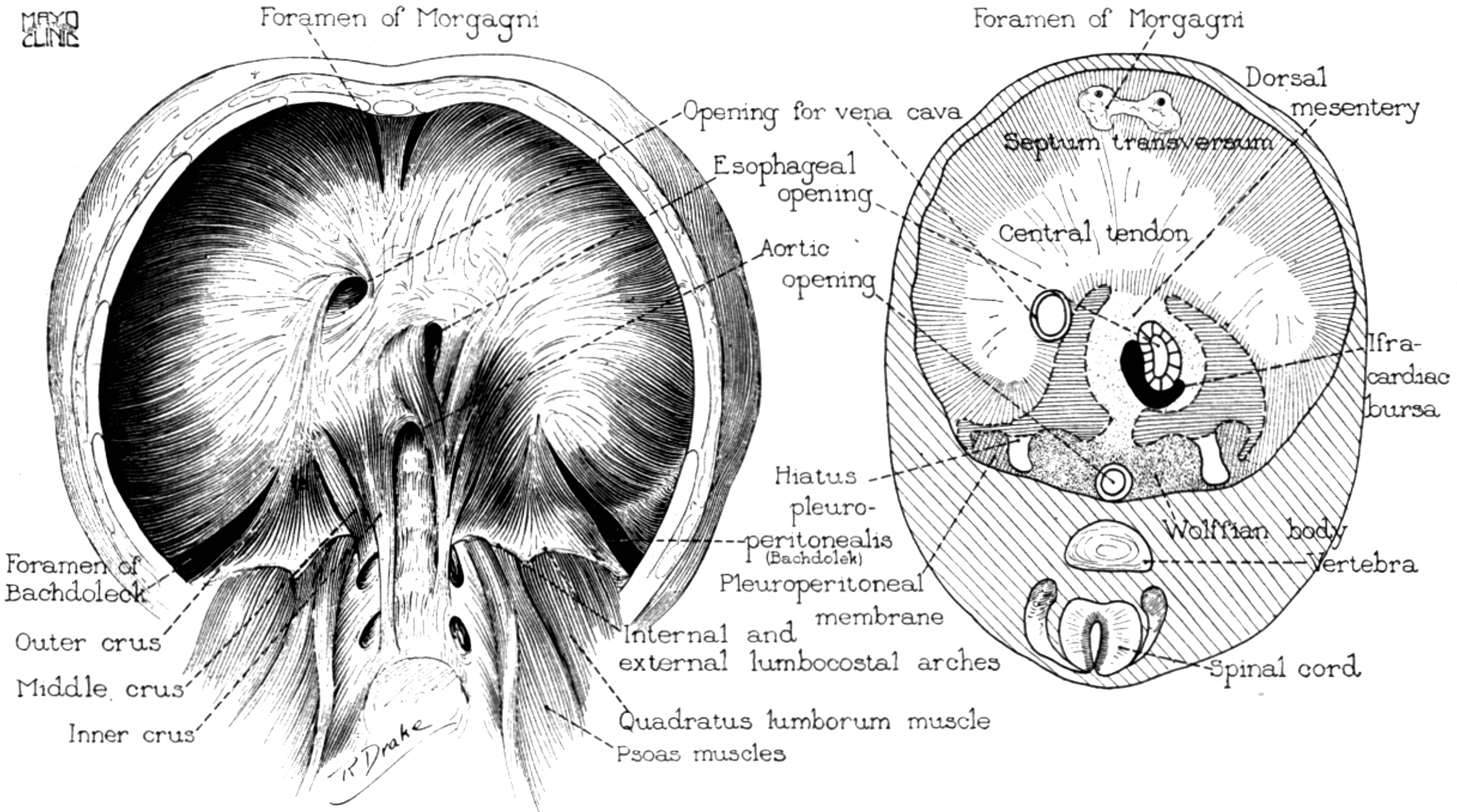
Foramen of Morgagni
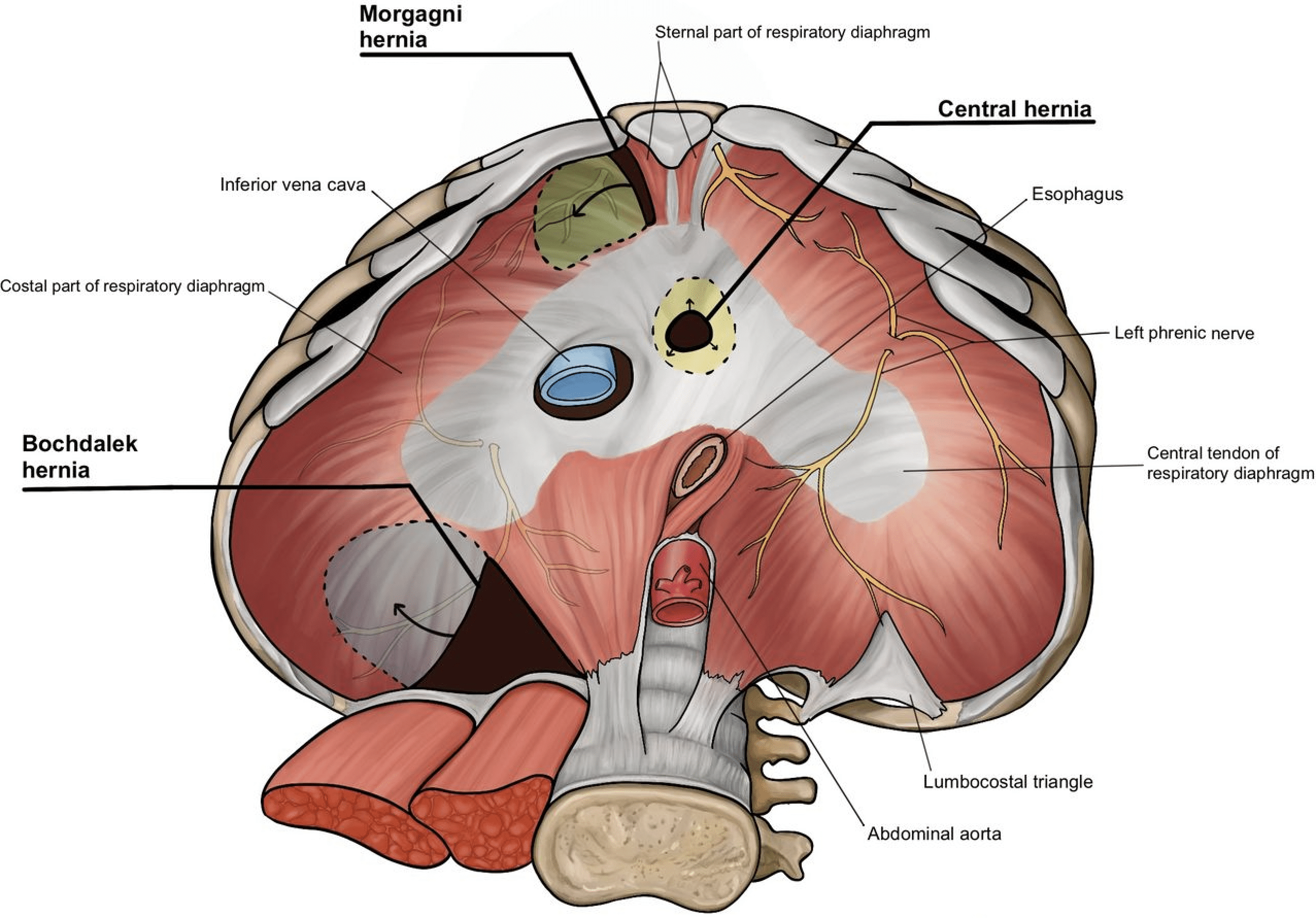
Anatomical weak spot between the sternal and costal portions of the diaphragm, prone to congenital defects. Though described by earlier anatomists, Morgagni’s Adversaria anatomica (1719) and De Sedibus (1761) provided detailed anatomical and pathological descriptions.
Morgagni hernia (1761)
Morgagni hernia is a congenital diaphragmatic hernia (CDH) accounting for 2–5% of CDH. An anterior, retrosternal congenital diaphragmatic defect through the sternocostal (parasternal) triangle (foramen of Morgagni). In comparison to Bochdalek hernia, a Morgagni hernia is more anterior and more often right-sided (~90%) and often discovered later in childhood or adulthood. Associated congenital anomalies are reported in 34–50%, especially cardiac defects (25–60%) and trisomy 21 (15–71%).
Frequently associated with a hernia sac, contents commonly include omentum and transverse colon, occasionally stomach, small bowel, or liver. Most patients are asymptomatic. Symptomatic cases present with chest/abdominal pain, dyspnoea, nausea/vomiting, or features of incarceration/volvulus.
Chest XR may show a paracardiac mass/air–fluid level at the right cardiophrenic angle. CT accurately defines the retrosternal defect and contents and can reach near-100% detection.
Repair is recommended for all due to incarceration risk; approach (open/laparoscopic; abdominal vs thoracic) is tailored to patient and contamination.
1761 – Morgagni first described the sternocostal gap in Tomus III, Liber IV, Epistola LIV, Article XI (“De vulneribus et contusionibus abdominis, lumborum, & membrorum”. he describes an anterior parasternal interval between xiphoid and adjacent fibres as a route for abdominal viscera into the thorax and also notes congenital diaphragmatic defects
Yet whenever the stomach is carried up through the diaphragm into the thorax, … there certainly are places in the diaphragm, through which… [a viscus] may pass over from the belly into the thorax… Thus also, anteriorly, betwixt the fibres that come from the xiphoid cartilage and the neighbouring fibres, there generally is an interval through which something similar may happen; and I even suspected this to have happen’d in a husbandman…
What symptoms an infant of two months old was troubled with… in whom, after death, almost all the intestines… were carried up into the thorax, through a foramen formed by nature in the diaphragm, on the left side of the foramen of the gullet…
Morgagni, 1761
1829 – Dominique-Jean Larrey, Baron de l’Empire (1766-1842) published De la hernie congéniale and discusses congenital diaphragmatic hernias in particular the anterior (parasternal) diaphragmatic hernia that later bore his name. Modern descriptions often differentiate right (Morgagni) from left (Larrey hernia) defects.
Key Medical Attributions
Morgagni and Pathological Anatomy
Morgagni’s De Sedibus (1761), documented over 700 clinicopathological correlations, and is considered a foundational text of pathological anatomy. It shifted medicine toward identifying the seat of disease in organs and tissues, rather than humoral imbalance.
Crohn’s disease (1761)
Crohn’s disease is a chronic, immune-mediated inflammatory bowel disease (IBD) characterized by transmural inflammation that can affect any part of the gastrointestinal tract, from the mouth to the anus.
1769 – Morgagni provided an early description of Ulceration of the intestines in De Sedibus et Causis Morborum. He describes the death and autopsy of a 20-year-old male patient who succumbed to a longstanding illness of fever, abdominal pain, and bloody diarrhoea. The autopsy revealed perforations and transmural inflammation with ulceration stretching from the terminal ileum to “two hands breadth” along the colon.
Original
English
Ileum vero, atque intestinum caecum, atque colon, mirum in modum affecta erant. Nam haec intestina non modo inusitata crassitie conspicua, sed & ulceribus scatentia, & in multis locis cohaerentia, atque stricta visa sunt; ita ut materiae faecales difficulter transirent. Quaedam ulcera in intimo tunicae situ ita profunda, ut pene ad peritonæum usque penetrarent. Praeterea abscessus in pariete intestini repertus est, ad quem fistula perduxit, quae in cavitatem abdominis aperta erat – Morgagni, De Sedibus, 1761, Epist. XXXIV, Art. IX (Vol. II)
The ileum, cecum, and colon were found to be extraordinarily diseased. For these intestines were not only remarkable for unusual thickening, but also were full of ulcers, and in many places were adherent and constricted, so that the faecal material passed with great difficulty. Certain ulcers extended so deep within the tunic that they nearly reached the peritoneum. Furthermore, an abscess was discovered in the intestinal wall, into which a fistula opened, which in turn communicated with the abdominal cavity – Morgagni, De Sedibus, 1761, Epist. XXXIV, Art. IX (Vol. II)
Stokes–Adams Attacks (1761)
Stokes-Adams syndrome refers to sudden, transient episodes of syncope resulting from intermittent complete heart block or severe bradyarrhythmia.
Morgagni described Stokes-Adams attacks in at least 2 sections of in De Sedibus et Causis Morborum, described several cases of sudden death and collapse linked to cardiac disease “a slow, unequal pulse preceded the sudden cessation of life.”
For example in De Morbis Capitis (letter IX, article 7); he details the case of the priest Anastasio Poggi:
He was in his sixty-eighth year, of a habit moderately fat, and of a florid complexion, when he was first seized with the epilepsy, which left behind it the greatest slowness of pulse, and in like manner, a coldness of the body.
Then in De morbis thoracis (letter LXIV, article V) regarding the case of a 64 year old merchant from Padua, a full-bodied man, who collapsed following vertigo
When visiting by way of consultation, I found with such a rarity of the pulse that within the 60th part of an hour the pulsations were only 22 – and this rareness which was perpetual – was perceived to be even more considerable, as often as even two (epileptic) attacks were at hand – so that the physicians were never deceived from the increase of the rareness they foretold a paroxysm to be coming on.
Morgagni 1761; LXIV(5): 505
Major Publications
- Morgagni GB. Nova institutionum medicarum idea, Patavii 1712.
- Morgagni GB. Adversaria anatomica: Prima; Tertia; Quarta; Quinta; Sexta. [Omnia; Altera]. 1719
- Epistolae anatomicae duodeviginti ad scripta pertinentes celeberrimi viri Antonii Mariae Valsalvae, Venetiis 1740.
- Morgagni GB. De sedibus, et causis morborum per anatomen indagatis. 1761 Tomus II; Tomus III [English translation: The seats and causes of diseases investigated by anatomy Book 2, Book 3. 1769]
- Opuscula miscellanea, Venetiis 1763.
- Opera omnia in quinque tomos divisa, [Bassano] 1764.
- Morgagni GB. The seats and causes of diseases investigated by anatomy (3 volumes: Translation by Benjamin Alexander) 1769. Vol II, Vol III
- Morgagni GB. The seats and causes of diseases, investigated by anatomy (2 Volumes: translation by William Cooke) 1882 Vol II
- Le epistole emiliane di Giambattista Morgagni volgarizzate per la prima volta, a cura di I. Bernardini, Forlì 1931.
- Consulti medici, a cura di E. Benassi, Bologna 1935.
- Le autobiografie, in Opera postuma, 1° vol., Roma 1964.
- Lezioni di medicina teorica, in Opera postuma, 2°-9° vol., Roma 1965-1993.
- Nova institutionum medicarum idea, a cura di L. Premuda, Padova 1982.
References
Biography
- Adams EW. Founders of Modern Medicine: Giovanni Battista Morgagni. (1682-1771). Med Library Hist J. 1903 Oct;1(4):270-7.
- Androutsos G. Giovanni-Battista Morgagni (1682-1773): creator of pathological anatomy. J BUON. 2006 Jan-Mar;11(1):95-101.
- Zani A, Cozzi DA. Giovanni Battista Morgagni and his contribution to pediatric surgery. Journal of Pediatric Surgery, 2008; 43(4): 729–733
- Morgagni, Giovanni Battista. Dizionario Biografico degli Italiani. 2012; 76
- Morgagni, Giovanni Battista. Il Contributo italiano alla storia del Pensiero: Scienze, 2013
- Zampieri F, Zanatta A, Thiene G. An etymological “autopsy” of Morgagni’s title: De sedibus et causis morborum per anatomen indagatis (1761). Hum Pathol. 2014 Jan;45(1):12-6.
- Öncel Ç, Baser S. Giovanni Battista Morgagni (1682-1771). J Neurol. 2016 May;263(5):1050-1052.
- Ghosh SK. Giovanni Battista Morgagni (1682-1771): father of pathologic anatomy and pioneer of modern medicine. Anat Sci Int. 2017 Jun;92(3):305-312.
- Aguirre Marco CP. Giovanni Battista Morgagni (1682-1771). Historia de la Medicina
Eponymous terms
- Larrey DJ. De la hernie congéniale In: Clinique chirurgicale, exercée particulièrement dans les camps et les hôpitaux militaires, depuis 1792 jusqu’en 1829. Tome III.
- Naumann G. Diaphragmatic Hernia; Laparotomy; Died, Hygiea 1888; 50: 524-528
- Walker EW. Diaphragmatic Hernia, with report of a case. The International journal of surgery, 1900; 13(9): 257-260
- Hedblom CA. Diaphragmatic hernia: A study of three hundred and seventy-eight cases in which operation was performed. JAMA 1925;85;(13):947-953.
- Harrington SW. Diaphragmatic hernia. Arch Surg. 1928;16(1):386–415.
- Flaxman N. The history of heart-block. Bulletin of the Institute of the History of Medicine. 1937; 5(2): 115-130
- Tarnay TJ. Diaphragmatic hernia. Ann Thorac Surg. 1968 Jan;5(1):66-92
- Hewitt WH. Archives of the forensic sciences: medicolegal contributions of historical interest. Miscellaneous minor works of Giovanni Battista Morgagni. Forensic Sci. 1972 Sep;1(3):339-87.
- Valvo JR, Cos LR, Cockett AT. Giovanni Battista Morgagni: his contributions to urology. Urology. 1983 Oct;22(4):452-7.
- Fogazzi GB. Kidney diseases in the major work of Giovanni Battista Morgagni. Nephrol Dial Transplant. 1998 Jan;13(1):211-2.
- Ventura HO. Giovanni Battista Morgagni and the foundation of modern medicine. Clin Cardiol. 2000 Oct;23(10):792-4.
- Eren S, Gümüş H, Okur A. A rare cause of intestinal obstruction in the adult: Morgagni’s hernia. Hernia. 2003 Jun;7(2):97-9. d
- Kesieme EB, Kesieme CN. Congenital diaphragmatic hernia: review of current concept in surgical management. ISRN Surg. 2011;2011:974041.
- Tubbs RS, Steck DT, Mortazavi MM, Shoja MM, Loukas M, Cohen-Gadol AA. Giovanni Battista Morgagni (1682-1771): his anatomic majesty’s contributions to the neurosciences. Childs Nerv Syst. 2012 Jul;28(7):1099-102.
- Slavec ZZ, Neudauer U. Marcus Gerbezius (1658–1718) and his first description of a complete atrioventricular block. Zdravniški vestnik 2015; 84(12): 855-860
- Pesce A, Frati A, Caruso R, Wierzbicki V, Raco A. Morgagni Spine Fractures-Dislocations per Anatomen Indagatis: Since the Dawn of Modern Medicine A Taxonomy and Pathomorphology Problem. World Neurosurg. 2016 Dec;96:171-176.
- Zampieri F, Zanatta A, Basso C, Thiene G. Cardiovascular medicine in Morgagni’s De sedibus: dawn of cardiovascular pathology. Cardiovasc Pathol. 2016 Nov-Dec;25(6):443-452.
- Lippi D. Gerbezius’ Pulsus Mira Inconstantia and the First Descriptions of the Atrioventricular Block. Cardiac Electrophysiology Clinics, 2018; 10(2): 179–1821
- Buttner R, Lee J. De-eponymising anatomical terminology. 2020
- Supomo S, Darmawan H. A rare adult morgagni hernia mimicking lobar pneumonia. Turk J Surg. 2022 Mar 28;38(1):98-100.
- Svetanoff WJ, Sharma S, Rentea RM. Morgagni Hernia. 2024 Aug 12. In: StatPearls [Internet].
- Kemerling MK, Okekumata I, Alasadi R, Cedeno-Rodriguez AR, Nuckton TJ. Right-sided Morgagni diaphragmatic hernia presenting as isolated left shoulder pain. BMJ Case Rep. 2024 Jun 22;17(6):e257631.
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |