
![]()
Grisel Syndrome
Description
Grisel syndrome: Non-traumatic rotatory atlantoaxial subluxation, with common causes being either infectious (mostly upper respiratory tract infections or retropharyngeal abscesses) or post-operative (following adenoidectomy, tonsillectomy or pharyngoplasty).
There are many proposed pathogenetic mechanisms for Grisel syndrome, with the most widely accepted theory being a two-hit hypothesis – the first hit being the existence of pre-existing ligament laxity, and a second hit from the induction of spasm caused by inflammatory mediators carried to the cervical muscles by the pharyngovertebral venous plexus.
Grisel syndrome primarily affects children, with only rare cases described in adults. Children and people with Down syndrome have a higher risk, and this is thought to be due to increased ligamentous laxity
Eponymously named after Pierre Grisel (1869–1959), a French paediatric surgeon who described the syndrome characterized by dislocation of the C1–C2 joint in patients with pharyngitis and torticollis in 1930
History of Grisel Syndrome
1830 – Sir Charles Bell first described a case of death from atraumatic atlanto-axial subluxation in a patient with probable syphilis and an ulcerating pharyngeal lesion
A patient, who had a deep ulcer in the back part of the throat, was seized with symptoms like those of apoplexy. These symptoms continued for two hours. At this time the patient’s head fell suddenly forward, and he instantly expired. On dissection, it was found that the ulcer had destroyed the transverse ligament, which holds the process of the dentata in its place. In consequence of the failure of this support, the process was thrown back, so as to compress the spinal marrow. The parts are preserved in my collection.
Bell, Case LXIV 1830
1875 – Eugène Dally (1833–1887), described 11 cases of torticollis, of which 4 were found to be due to an acute infectious disease. One case in particular, describes a 12 year old girl who is diagnosed with acute rheumatic fever evidenced by St Vitus dance (Sydenham’s chorea) which Dally localises to disease at the atlanto-occipital level
1919 – Harold Swanberg (1891-1970) published a case report in JAMA 1919 of a non-traumatic atlas dislocation occurring in a 22 year old soldier initially presenting to a military base hospital suffering from measles and acute follicular tonsillitis in December 1917. Tonsillectomy was performed on January 16, 1918 but on the night of the operation the patient’s neck suddenly became stiff. He was transferred to General Hospital No. 6, in July, 1918 with the following brief history:
“1. Complaint: Pain in neck, stiffness of cervical muscles which permits of very little motion of the head, except anterior-posteriorly, which motion is limited. 2. Search for focal infection: (a) Tonsils (fragments); (b) roentgen ray, ostearthritis, first and second cervical vertebrae; 3. Treatment: (a) Tonsil fragments removed; (b) specimen from tonsil shows gram-negative diplococci; removed; Condition on dismissal: No improvement. Etiology: Probably of focal origin (tonsils).“
On examination; the neck was stiff, all motions being resisted in every direction; the soldier held his head in a rigid position with the chin depressed; he complained of pain in the cervical muscles on motion attempted in any direction; he could not rotate his head; he had persistent headaches.
This case is so unusual, both as to the etiology and the failure to recognize the condition [atlas dislocation] for a long period, that it is well worth reporting.
Swanberg 1919
1930 – Pierre Grisel (1869-1959) publishes a case report of two children involving non-traumatic atlanto-axial dislocation following tonsillectomy and nasopharyngitis in 1930 in La Presse Médicale.
Original
English
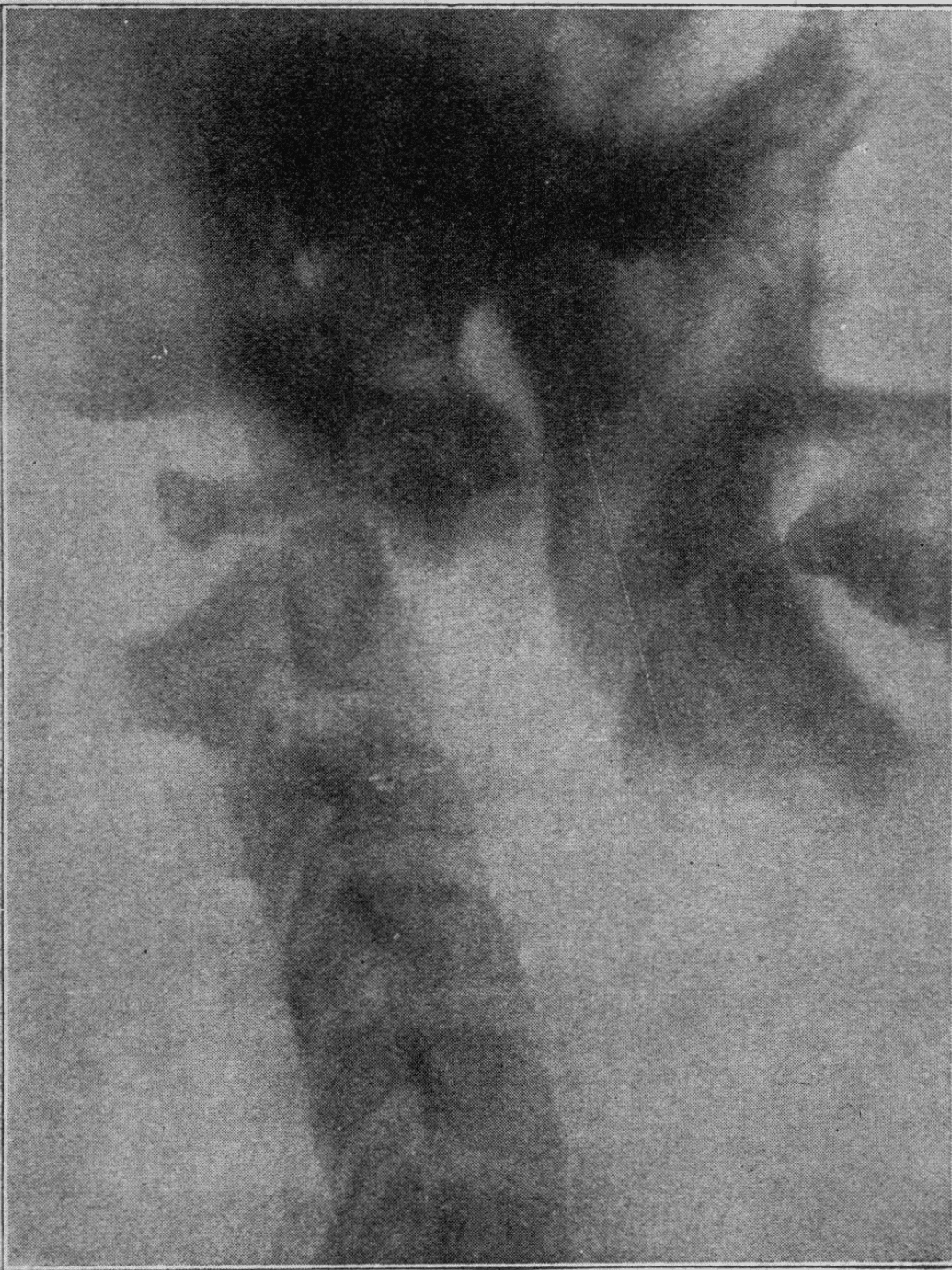
Fig 3. Observation II. Radiographie de profil des articulations sous-occipitales
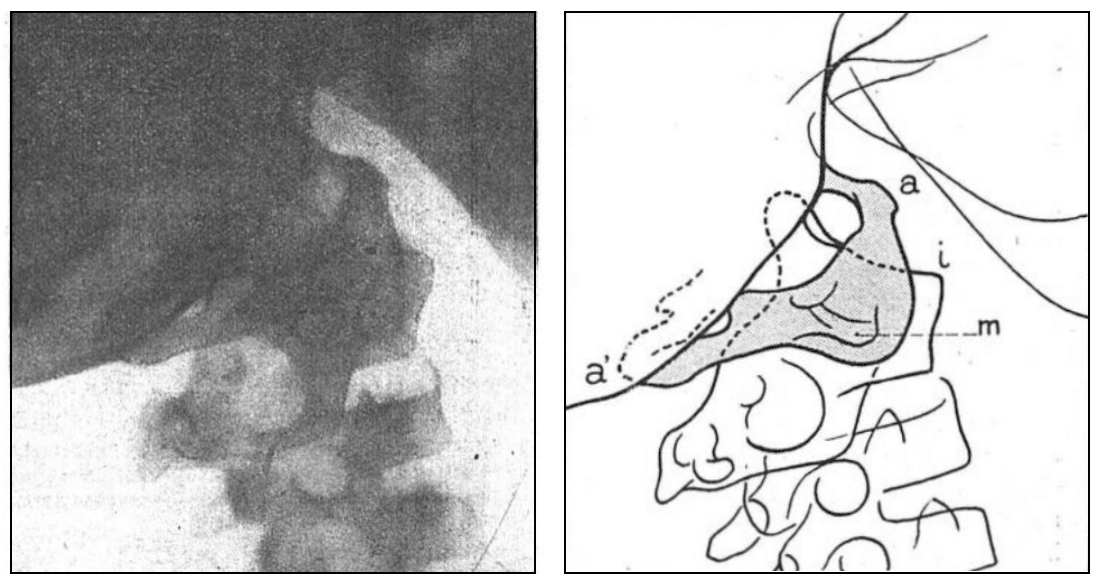
Fig 3 bis. Observation II. Schéma de la Fig 3. On voit en (i) l’angle de la surface articulaire droite de l’axis, complètement abandonnée par la masse laterale correspondante reportée en arrière, les tubercules antérieurs et postérieurs de l’atlas, (a) et (a’), et sa masse latérale gauche (m) qui a été chassée par la compression et la traction en bas et an avant au devant du corps de l’axis. La partie de l’atlas non cachée par la base du crane est seule teintée en gris
Fig 3. Observation II. Profile x-ray of the suboccipital joints
Fig 3a. Observation II. Diagram of Fig 3. We see in (i) the angle of the right articular surface of the axis, completely abandoned by the corresponding lateral mass carried back, the anterior and posterior tubercles of the atlas, (a) and (a’), and its left lateral mass (m) which has been driven out by compression and traction down and forward in front of the body of the axis. The part of the atlas not hidden by the base of the skull is only tinted in grey
This 1930 edition of La Presse Médicale also had the first eponymous reference to de maladie de Grisel (Grisel’s syndrome), where Grisel’s colleague Desfosses reports a case of nasopharyngeal torticollis:
Original
English
Les parents avaient à peine commencé l’histoire de la malade que je les arrêtais : « Je vais, leur dis-je, vous lire des observations qui viennent de paraître dans La Presse Médicale, elles vout vous éclairer de suite sur le torticolis de votre fille.
En elfet, un court article de mon excellent ami P. Grisel sur le Torticolis naso-pharyngien, paru le 11 Janvier 1930 dans La Presse Mėdicale, nous permettait de reconnaître du premier coup d’æil et au simple récit des accidents initiaux l’affection dont était
atteinte, depuis 2 mois, cette fillette. L’examen des radiographies confirma cette e opinion a priori. Pour plus de súreté sur l’exactitude du diagnostic, le bon sens, la bonne camaraderie, la bonne justice exigeaient que l’ami Grisel füt appelé en consultation. Deux jours plus tard, nous nous trouvions avec lui et avec le médecin traitant chez la petite malade et nous půmes à loisir, de concert, fignoler le diagnostic.
The parents had hardly begun the story of the patient when I stopped them: “I am going to read to you some observations which have just appeared in La Presse Médicale, they will enlighten you immediately on the torticollis of your daughter.
In fact, a short article by my excellent friend P. Grisel on nasopharyngeal torticollis, which appeared on 11 January 1930 in La Presse Médicale, enabled us to recognise at a glance, and from the simple account of the initial incidents, the condition with which this daughter had been suffering for two months.The examination of the X-rays confirmed this a priori opinion. To be sure of the accuracy of the diagnosis, common sense, good fellowship, and good justice demanded that our friend Grisel be called in for consultation. Two days later, we were with him and the attending physician at the little patient’s home and we were able to fine-tune the diagnosis together
Associated Persons
- Charles Bell (1774-1842)
- Arnold Wittek (1871-1956)
- Eugène Dally (1833–1887)
- Pierre Grisel (1869-1959)
- William Harold Swanberg (1891-1970)
Alternative names
- Grisel’s syndrome; La maladie de Grisel
- Distensionsluxation (Wittek)
- Drehungsverrenkung (Sudek)
- Inflammatory dislocation (Fitzwilliams)
- Non-traumatic subluxation (Berkheiser & Seidler)
- Spontaneous dislocation (Hess)
- Spontaneous hyperaemic dislocation (Watson-Jones)
- Le faux torticollis aigu (Moyson & Watticz)
- Altlantoaxial rotation
- Nontraumatic rotatory subluxation of the atlantoaxial joint; Nontraumatic atlantoaxial subluxation
Controversies
There were many descriptions of non-traumatic atlanto-axial dislocations prior to Grisel’s work in 1930, including both infectious and post-operative aetiologies. Despite this, the eponymous term was quickly accepted as the correct term – particularly in the French literature. Additionally, Persian and Greek physicians may have provided some the earliest descriptions of what is now referred to as Grisel syndrome. As early as the tenth century, Hidayat al-Muta`allemin fi al-Tibb (The Students’ Handbook of Medicine) described a complication of diphtheria associated with neck pain and subluxation of the cervical vertebrae
References
Historical references
- Bell C. Case LXIV. In: The nervous system of the human body. 1830: 391
- Dally E. Du torticolis occipito-atloïdien. Bulletin général de thérapeutique médicale et chirurgicale. 1875; 89: 354-356
- Wittek A. Ein Fall von Distensions luxation im Atlanto-epistropheal-Gelenke. Münchener medizinische Wochenschrift. 1908; 55: 1836-1837
- Swanberg H. Anterior dislocation of atlas following tonsillectomy. JAMA. 1919; 72(2): 107-108
- Grisel P. Enucléation de l’atlas et torticolis naso-pharyngien. La Presse médicale, 1930; 38: 50-53
Eponymous term review
- Wetzel FT, La Rocca H. Grisel’s syndrome. Clin Orthop Relat Res. 1989 Mar;(240):141-52.
- Osiro S, Tiwari KJ, Matusz P, Gielecki J, Tubbs RS, Loukas M. Grisel’s syndrome: a comprehensive review with focus on pathogenesis, natural history, and current treatment options. Childs Nerv Syst. 2012 Jun; 28(6):821-5.
- Golzari SE, Ghabili K, Sajadi MM, Aslanabadi S. Early descriptions of Grisel’s syndrome. Childs Nerv Syst. 2013 Mar;29(3):359-60.
- Ciftdemir NA et al. A Rare Case of Torticollis: Grisel Syndrome. Journal of Tropical Pediatrics. 2018; 64: 245-248
- Anania P et al. Grisel Syndrome in Pediatric Age: A Single-Center Italian Experience and Review of the Literature. World Neurosurg. 2019 May; 125: 374-382.
- Pini N, Ceccoli M, Bergonzini P, Iughetti L. Grisel’s Syndrome in Children: Two Case Reports and Systematic Review of the Literature. Case Rep Pediatr. 2020 Nov 12; 2020: 8819758
- Fox SM. Nontraumatic AtlantoAxial Subluxation in Children. PedEMmorsels
eponymictionary
the names behind the name
BSc, MD (UWA), MPH (UNSW). Emergency Physician in training. German translator and lover of medical history.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
