
![]()
Pierre Grisel
Pierre Adolph Grisel (1869-1959) was a French paediatric ENT surgeon
Eponymously remembered for his description of spontaneous, nontraumatic rotatory subluxation of the atlantoaxial joint following peripharyngeal inflammation or otorhino-laryngologic surgical procedures, or Grisel syndrome, in 1930
Very little is known about the life, times and works of Grisel the surgeon.
Biography
- Born on October 21, 1869 in Paris
- Chef de Clinique chirurgicale infantile
- Died on October 24, 1959 in Paris aged 90
Medical Eponyms
Grisel syndrome (1930)
Spontaneous, nontraumatic rotatory subluxation of the atlantoaxial joint following peripharyngeal inflammation or otorhino-laryngologic surgical procedures (e.g. tonsillectomy, adenoidectomy). Occurs most commonly in the pediatric population
1830 – Charles Bell was the first to describe this syndrome
1930 – Grisel described and published cases of two children. It’s a rare clinical presentation which, in a febrile context, associates an acute torticollis linked to a contracture of the cervical pre- and peri-vertebral muscles due to an inflammation or infection of the nasopharynx or the retropharyngeal space, and this without any notion of bone pathology or trauma. It is accompanied by a rotatory subluxation of the atlas.
In his publication Grisel wrote:
The torticollis sometimes leaves behind a definitive vicious attitude. It is then one of its characterized, in its acute period, by the acuteness of the infection, of the deviation of the head and of the neck, of the evolution, and, in its chronic period, by a set of typical deformations, not progressive, but on the contrary appeared from the beginning with their degree and their definitive character.
A little girl of about ten years old, a few hours after a removal of tonsils or vegetations, at the beginning of an angina, is taken of high fever with pharyngeal pain and torticollis with extreme of torticollis with extreme deviation. After a few days, the temperature is normalized, the neck becomes deflects and palpation reveals the presence of retro-angulo-maxillary ganglions which are still painful. The cervical pain, high at the beginning, diminishes or disappears as well as the adenopathy, but a vicious attitude persists, all the more apparent as it is located in the sub-occipital region.
A real drama with rapid events took place there, which in a few days made a child a few days, of a child until then well conformed, a child whose deformity appears to all eyes. […] A spontaneous or postoperative infection […] determines in the retropharyngeal space an acute lymphangitis […] which, extending to the second lymph node, becomes visible and palpable in the visible and palpable in the internal jugular chain […].
The irreducibility is not due to to a simple snag that a rapid intervention could release, but to the permanent contracture at the beginning, to the fibrous retraction afterwards, which immobilizes the dislocated atlas and opposes its to its reinstatement by maintaining the abnormal approach of the occipital and the axis […]. It is the the abrupt dislocation of the atlas that makes, from the initial acute period, the torticollis definitive
Original
English
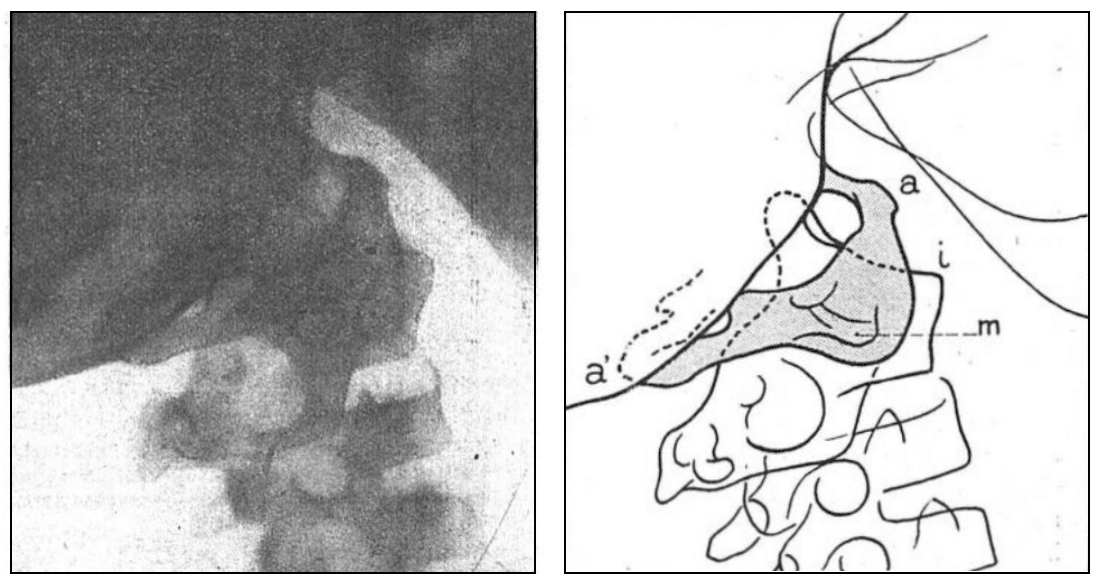
Fig 3. Observation II. Radiographie de profil des articulations sous-occipitales
Fig 3 bis. Observation II. Schéma de la Fig 3. On voit en (i) l’angle de la surface articulaire droite de l’axis, complètement abandonnée par la masse laterale correspondante reportée en arrière, les tubercules antérieurs et postérieurs de l’atlas, (a) et (a’), et sa masse latérale gauche (m) qui a été chassée par la compression et la traction en bas et an avant au devant du corps de l’axis. La partie de l’atlas non cachée par la base du crane est seule teintée en gris
Fig 3. Observation II. Profile x-ray of the suboccipital joints
Fig 3a. Observation II. Diagram of Fig 3. We see in (i) the angle of the right articular surface of the axis, completely abandoned by the corresponding lateral mass carried back, the anterior and posterior tubercles of the atlas, (a) and (a’), and its left lateral mass (m) which has been driven out by compression and traction down and forward in front of the body of the axis. The part of the atlas not hidden by the base of the skull is only tinted in grey
Major Publications
- Grisel P, Dévé F. L’abcès ossifluent hydatique d’origine vertébrale: Le mal de Pott hydatique. 1900
- Grisel P. Des malformations rachitiques du membre inférieur chez l’enfant. 1900
- Grisel P. Contribution a l’étude des malformations rachitiques du membre inférieure chez l’enfant. Thèse de Paris 1900
- Grisel P. De l’Invagination intestinale de l’enfant. IVe Congrès périodique de gynécologie, d’obstétrique et de paediatrie, 1904
- Grisel P. Enucléation de l’atlas et torticolis naso-pharyngien. La Presse médicale, 1930; 38: 50-53
- Grisel P. Félix Dévé. La Presse médicale, 1951 Dec 08; 59(78): 1647-8
Controversies
Potential: Docteur Pierre GRISEL 1869-1959. Source: Grave of Grisel (Père-Lachaise, division 47)
References
Biography
- Pierre Grisel. La Presse Médicale. 1959; 61: 2365
- Falcimaigne A. Pierre Adolphe GRISEL. Geneanet
- Pierre Grisel (1874-1959). BNF Data
- Bibliography. Grisel, Pierre. WorldCat Identities
Eponymous terms
- Golzari SE, Ghabili K, Sajadi MM, Aslanabadi S. Early descriptions of Grisel’s syndrome. Childs Nerv Syst. 2013 Mar;29(3):359-60.
- Cadogan M. Sir Charles Bell (1774 – 1842). LITFL
Eponym
the person behind the name

Prof. Nicolas Peschanski currently works as a Consultant in Emergency Medicine at the Urgences Adultes-SAMU-35 SMUR, Centre Hospitalier Universitaire de Rennes. Nicolas does research in Emergency Medicine at U1096 INSERM EnVI Normandy University research Unit. He's Associate Prof. teaching Clinical Medicine and Emergency Medicine at Rennes-1 University School of Medicine. Involved in the #FOAMed development, he is a current member of the french Society of Emergency Medicine Guideline Committee.
BSc, MD (UWA), MPH (UNSW). Emergency Physician in training. German translator and lover of medical history.