![]()
High Pressure-Injection Injury
aka Trauma Tribulation 009
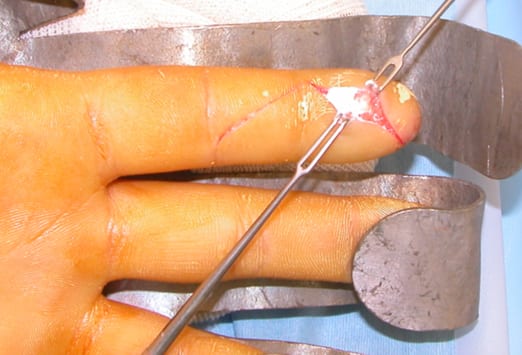
A 43 year-old male presents to the emergency department with a 2 hour history of a sore, swollen palm since injuring his hand with the spray from a paint gun he was using to paint his driveway.
On examination, you notice a small pin-hole sized entry wound to the palmar surface of his left hand with mild localised erythema. He has good range of movement throughout the joints of the hand is neurovascularly intact. Palpation reveals only mild localised tenderness.
Does he need anything more than a reassuring pat on the back and discharge home?

Questions
Q1. What is the Diagnosis?
Answer and interpretation
High-pressure injection injury to the hand.
- High-pressure injection injuries are caused by the accidental injection of fluid from high pressure industrial equipment such as hydraulic systems or paint spraying devices.
- High-pressure injection injures are a surgical emergency.
- Most commonly occur in occupational settings.
- High pressure injection guns are used for many tasks such as painting, lubricating, greasing, cleaning and the mass inoculation of animals.
- Injury generally occurs in young males and affect the non-dominant hand: commonly the index finger, followed by middle finger and palm. Injury generally results in people with limited experience using these devices.
- Common materials found in high-pressure injuries are:
- Paint (60%)
- Grease (25%)
- Water
- Oil
- Diesel
- Paint thinner
- Animal vaccines

Q2. What is the mechanism of injury caused by high-pressure injection guns?
Answer and interpretation
- High-pressure guns emit jet streams at pressures of up to thousands of psi. At these extreme pressures, material is forced through the skin and may track along fascial planes, tendon sheaths, and neurovascular bundles.
- Although high-pressure injection injuries are relatively uncommon, they may occur easily because as only 100psi is sufficient pressure to breach the skin.
- Even small amounts of contaminants injected into the skin can lead to compartment syndrome, poor perfusion and closed spaced infection of the anatomical spaces and tendon sheaths.
Tissue injury from high-pressure injection is dependent on the following factors:
- Type of material injected
- Amount injected
- Anatomical location
- Velocity of injected material
Q3. How do high-pressure injection injuries present to the ED?
Answer and interpretation
Patients generally give a history of coming into close contact with the jet stream during either the clearing or cleaning of the nozzle, or during general use of the device.
Early examination generally reveals no apparent break in the skin or a benign-appearing pinhole-sized puncture wound with minimal symptoms. Symptoms generally develop over 4-6 hours as the digit/extremity becomes swollen, painful and pale.
Classified into 3 stages:
1. Acute Stage
- Occurs with 4-6 hours
- Symptoms include swelling, anaesthesia and vascular insufficiency
- Without prompt treatment the digit/extremity will succumb to tissue ischaemia and necrosis by 12 hours
- Rarely systemic absorption can occur from the foreign material causing a generalised toxic reaction characterised by lymphagitis, leukcytosis and fever.
2. Intermediate Stage
- Is characterized by the development of oleomas (lipogranulomas) at the injection site and throughout the affected tissues.
- The reaction to the foreign material in the tissues make the body prone to the development of these nodular tumors.
- The oleomas generally remain dormant, however can become fibrosed resulting in functional loss.
3. Late Stage:
- The late stage is characterized by the breakdown of the skin integrity over the oleomas leading to ulcer and sinuses formation resulting in secondary infection.

Q4. What is the appropriate management in the ED?
Answer and interpretation
Emergency department management starts with the clinician being able to recognise the seriousness of this injury, initiate prompt aggressive management and arrange for urgent review by a hand surgeon.
“The mainstay of treatment involves surgical decompression, removal of the foreign material,and debridement of the necrotic tissue.”
The following steps can be taken to improve outcomes while the patient is in the emergency department:
- Developing of pain is a worrying sign provide effective analgesia via the oral or parenteral route. Digital nerve blocks are not recommended as will increase compartment pressures and alter ongoing examination of the digit.
- Initiate broad spectrum antibiotics to cover for both gram negative & positive organisms (consult local/institutional guidelines)
- Arrange for imaging:
- X-ray is the imaging of choice
- Help determine dispersion and thus extent of exploration required
- Lead-based paints appear as soft tissue densities (avoid confusing with calcification)
- Non-lead-based paints appear as subcutaneous emphysema
- Grease will appear as a lucency
- The use of steroids to reduce inflammation from the foreign material has shown promise in animal studies, however some clinicians are concerned regards the risk of increasing infection rates from the use of steroids.
- Check patients tetanus status and update accordingly
- Urgent consultation with a hand specialist for early decompression, debridement and washout is required.
- Keep patient NBM and prepare for theatre
- Even if debridement occurs within 6 hours for paint thinner, jet fuel, petrol, or oil the amputation rate is still 38%, compared to 58% amputation rate when treatment occurs over 6 hours. High caustic agents like turpentine and paint solvents, along with higher injection pressures have an amputation rate of about 80% even with appropriate care.
- Of the injuries that don’t result in amputation most will have some form of long-term functional impairment and patients should be counseled accordingly.
{kind=link}
{kind=link}
Take home points!
- Never judge a book by its cover!!! Don’t be fooled by benign-appearing high-pressure injection wounds.
- Provided broad spectrum antibiotics early
- Consult hand surgeon as soon as you suspect high-pressure injection injury.
- Educate patient of the high likelihood of some level of dysfunction despite adequate treatment.
References
- Loveday, I. (2007). High-pressure injection injuries. Emergency Nurse. PMID: 18065043
- Locker, J. & Carstens, A. (2010). High-pressure injection of silica-based paint into a finger. The New Zealand Medical Journal. PMID: 20648104
- Kohli, N. (2009). High-pressure injection injury in a furniture repairman -an outwardly minor in jury with the potential for a devastating outcome. Journal of Occupational and Environmental Medicine. PMID: 19741372
CLINICAL CASES
Trauma Tribulation
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC