
![]()
Hyperkalaemia Clinical Case
Case Study of Hyperkalaemia:
George is a 72 year old male found collapsed at home on floor of his bedroom, incontinent of urine and faeces. He complained of significant pain in his right hip with shortening and rotation. George’s family last had contact with George 3 days prior to his collapse.
Assessment:
- On arrival at ED he is confused and combative with a GCS 0f 13
- Initial observations reveal BP 78/60; Pulse 74, RR 32, SPO2 91% (NRB 15L)
- ABG which shows a Potassium of 9.0, pH of 7.23 and a Blood Glucose Level of 32mmol
Medical History:
- CCF
- Hypertension
- Type 2 DM
- Osteoarthritis
Medication History:
- George is taking enalapril for hypertension; spironolactone & metoprolol for his CCF and celebrex for his osteoarthritis
- His diabetes is diet controlled.
An ECG is performed on his arrival to the resuscitation area…
You briefly review the ECG and confidently state (already knowing the ABG result) that this patient has sever hyperkalemia. Brilliant…now what?
The 5 C’s of Metabolic Disturbances
I use the 5 C’s approach to recognise, understand and manage metabolic disturbances in the ED.
- Causes – Understanding normal metabolic homeostatic mechanisms helps define potential causative events that lead to disruption of the sensitive pathophysiological milieu. Increased production; increased intake and decreased excretion are often the commonest causal factors in metabolic disruption.
- Clinical manifestations – evaluate, recognise and diagnose the problem
- Complications – what can go wrong in the short, medium and long term can define clinical manifestation, duration of illness and potentially affect management decisions
- Calculations – Calculate to Obviate
- Corrective measures – Call to action…how do you actually fix the problem!
Potassium Pathophysiology
- Serum potassium is normally maintained between 3.5 -5.0 mmol/L
- Hyperkalaemia is defined as a potassium level greater than 5.5 mmol/L
- Hyperkalaemia is a potentially life-threatening metabolic problem caused by inability of the kidneys to excrete potassium, impairment of the mechanisms that move potassium from the circulation into the cells, or a combination of these factors.
Classic Causes of Hyperkalaemia
- Excessive exogenous potassium load (Increased Intake)
- Potassium supplements (IV or Oral)
- Excess in diet
- Salt substitutes (e.g. potassium salts of penicillin)
- Excessive endogenous potassium load (Increased Production)
- Haemolysis
- Rhabdomyolysis
- Extensive burns
- Tumor Lysis Syndrome
- Intense physical activity
- Trauma (especially crush injuries and ischaemia)
- Redistribution (Shift from intracellular to extracellular fluid)
- Acidosis (metabolic or respiratory)
- Insulin deficiency
- Drugs
- Succinylcholine
- Beta-blockers
- Digoxin (acute intoxication or overdose)
- Hyperkalaemic familial periodic paralysis
- Diminished potassium excretion (Decreased Excretion)
- Decreased glomerular filtration rate (eg, acute or end-stage chronic renal failure)
- Decreased mineralocorticoid activity
- Defect in tubular secretion (eg, renal tubular acidosis IV)
- Drugs (eg, NSAIDs, cyclosporine, potassium-sparing diuretics, ACE Inhibitors)
- Pseudohyperkalemia (Factitious)
- Haemolysis (in laboratory tube) most common
- Thrombocytosis
- Leukocytosis
- Venepuncture technique (e.g. prolonged tourniquet application)
Clinical Manifestations
Signs and Symptoms of Hyperkalaemia:
- Clinical features are often non specific
- Generalised muscle weakness
- Flaccid paralysis and paraesthesia of the hands and feet
- Lethargy, Confusion, Weakness and Palpitations
ECG Changes of Hyperkalaemia:
- The ECG is one of the most important diagnostic tools in detecting hyperkalaemia
- Predicted ECG changes associated with Hyperkalaemia include
| Serum Potassium (mmol/L) | Predicted ECG status |
| 5.5-6.5 | Tall tented T waves |
| 6.5-7.5 | Loss of P wave |
| 7.5-8.5 | Widening QRS |
| >8.5 | QRS continues to widen, approaching to sine wave |
ECG Changes of Hyperkalaemia:

Early ECG changes showing Peaked T waves
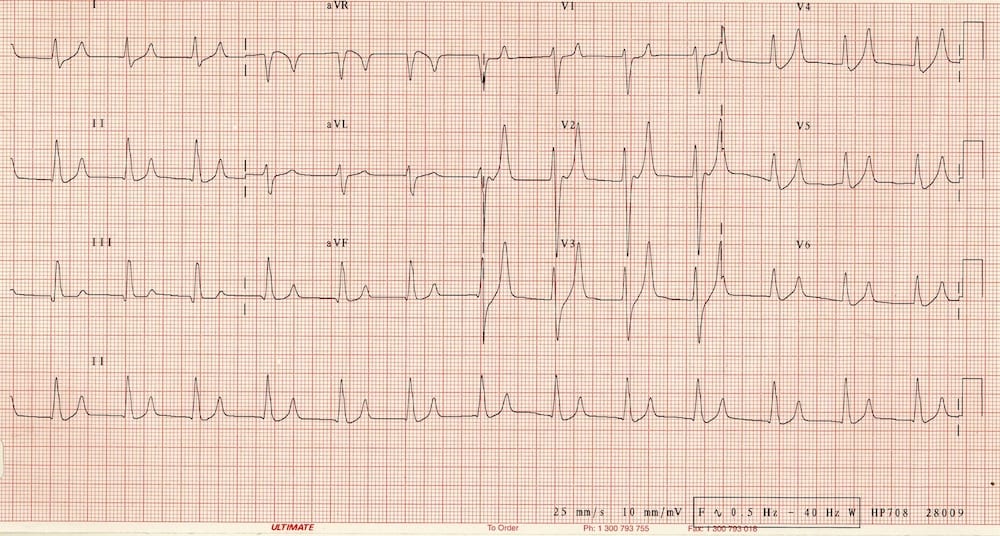
ECG of patient with Potassium of 8.5 mmol/L

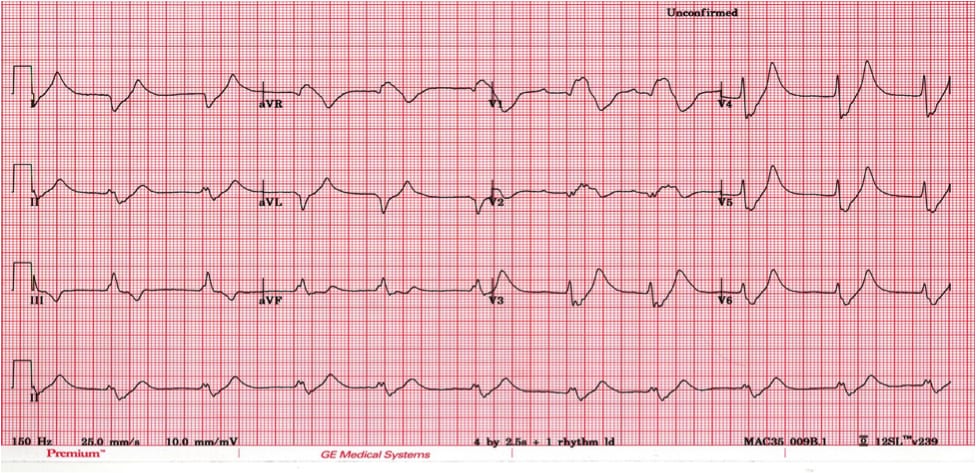
Potassium of 9.0mmol/L on 12 lead ECG.
Management of Hyperkalaemia
Treatment of hyperkalaemia involves stabilizing the myocardium to prevent arrhythmias, shifting potassium back into the intracellular space and removing excess potassium from the body.
1. Correct Serious Conduction Abnormalities (Calcium)
- Calcium is a very useful agent. It does not lower the serum potassium level, but instead is used to stabilise the myocardium, as a temporising measure. Calcium is indicated if there is widening of QRS, sine wave pattern (when S and T waves merge together), or in hyperkalaemic cardiac arrest.
- The ‘cardiac membrane stabilising effects’ take about 15-30mins.
- Calcium Chloride
- Dose: Calcium Chloride 10% 5-10mL
- 3 x more potent than Calcium gluconate
- Complication: severe thrombophlebitis
- Calcium Gluconate:
- Dose: Calcium gluconate 10% 5-10mL
- Less potent, less irritating to veins
- Potential Complications of Calcium administration
- Bradycardia, hypotension and peripheral vasodilation
- Generally these occur if administered too quickly
- Avoid in digoxin toxicity (use magnesium as alternative)
2. Drive Potassium into the Cell:
- Insulin & Glucose
- Dose: IV fast acting insulin (actrapid) 10-20 units and glucose/dextrose 50g 25-50ml
- Insulin drives potassium into cells and administering glucose prevents hypoglycaemia.
- Begins to work in 20-30mins reduces potassium by 1mmol/L and ECG changes within the first hour
- Sodium Bicarbonate
- Dose: 50- 200mmol of 8.4% Sodium Bicarbonate
- Bicarbonate is only effective at driving potassium intracellularly if the patient is acidotic
- Begins working in 30-60 minutes and continues to work for several hours.
- Salbutamol
- Dose: 10-20mg via nebulizer
- Beta 2 agonist therapy lower K via either IV or nebulizer route.
- Salbutamol can lower potassium level 1mmol/L in about 30 minutes, and maintain it for up to 2 hours.
- Very effective in renal patients that are fluid overloaded
3. Eliminate Potassium From the Body:
- Calcium resonium
- Dose: 15-45g orally or rectally, mixed with sorbitol or lactulose
- Calcium polystyrene sulfonate is a large insoluble molecule that binds potassium in the large intestine, where it is excreted in faeces
- Effects take 2-3 hours
- Frusemide
- Dose: 20-80mg depending on hydration status
- Potassium wasting diuretic. Helps to urinary excrete potassium in conjunction with hydration or fluid overloaded patients
- Normal Saline
- Used to help renally excrete potassium, by increasing renal perfusion and urinary output. Cautious use in patients with renal & heart failure
- Dialysis
- Is the gold standard for removing potassium from the body. Provides immediate and reliable removal.
- Can lower potassium by 1mmol/L in first hour and another 1mmol/L over the next 2 hours.
References and Links
LITFL
- CCC – Hyperkalaemia management
- CCC – Hyperkalaemia DDx
- CCC – Hypokalaemia
- CCC – Hypokalaemia Mind Map
- ECG Library – Hyperkalaemia
- ECG Library – Hypokalaemia
- Clinical Case – Hyperkalaemia
Hyperkalaemia even affects ER Consultants!!!

Critical Care
Compendium
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |