
![]()
ICE 011: Tall Story
An 83 year old man with a past history of Type 2 diabetes, hypertension and ischaemic heart disease has become progressively unwell over the last 5 days. His GP discovered a pneumonia on CXR and has been treating him with oral antibiotics for the last 3 days but his clinical condition has continued to worsen.
Observations: HR 90 /min, BP 115/70 mmHg and Temp 37.6 °C, RR 20 /min, with O2 saturation 91% (room air)
Questions
- What does the ECG show ?
- What urgent treatment is needed for the condition shown on the ECG ?
Reveal the ICE answer
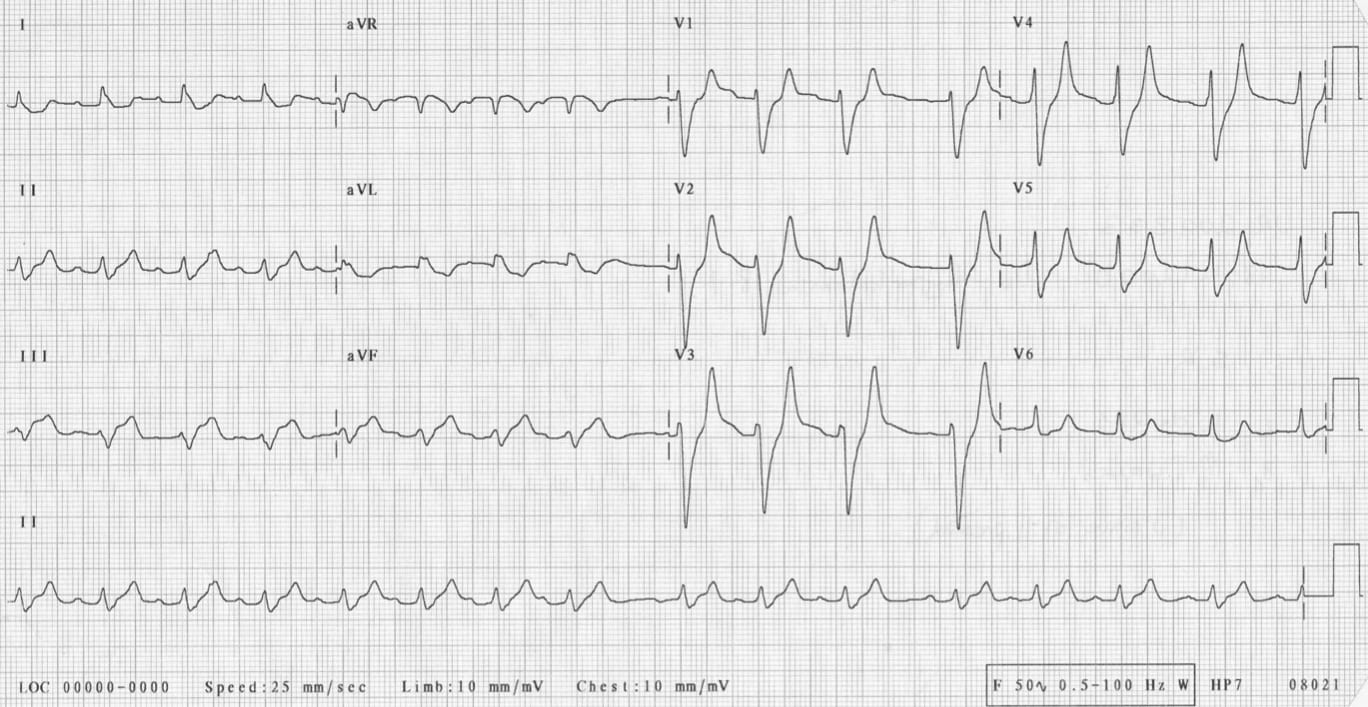
This ECG shows most of the classic features of severe hyperkalaemia. Given the clinical scenario this is likely due to renal failure secondary to sepsis. In particular the ECG shows:
- Sinus rhythm at 90 /min
- T waves peaking or tenting
- PR segment lengthening to 220 msec
- QRS widening
It is very likely that his serum K+ is above 7.5mmol/L with these findings. This is a life threatening situation. If his K+ rises more his ECG will become a “sine wave” before deteriorating into ventricular fibrillation then asystole.
As well as treating any reversible cause (in this man, renal failure and sepsis ), think of the treatment for severe hyperkalaemia in 3 parts:
- Protect the heart from malignant arrhythmias
– Calcium chloride or gluconate (10mls of 10%) - Move the K+ into cells
– Salbutamol nebulised (5 or 10mg)
– Glucose (50mls 50%) + Insulin (5 to 10U)
– NaHCO3 (50mls of 8.4%) - Enhance excretion of K+ from the body
– Resonium orally or rectally
– Haemodialysis
Further reading:
- ECG Library – Hyperkalemia
- BSCC – ECG waves and hyperkalaemia
- CCC – Hyperkalaemia Management
- Cases – Hyperkalaemia Clinical Case

ICE CASES
Ian’s clinical emergencies
emergency physician keen on medical education and cycling