
![]()
José Luis Bado

José Luis Bado (1903-1977) was a Uruguayan surgeon.
Bado published 130 scientific papers and 12 books. He founded the Instituto Traumatologico de Montevideo (Instituto de Ortopedia y Traumatologia) and single handedly brought the practice of orthopedic surgery to Uruguay and across South America.
Bado wrote his seminal book: ‘The Monteggia Lesion’ in 1962 in which he further classified the Monteggia injury in to four types (rather than just the one extension type described by Giovanni Monteggia 155 years earlier)
Bado published his research on ‘The Monteggia Lesion’ in 1967 and reported the treatment outcomes of 22 adults and 18 children advocating non operative treatment in all but type IV injuries. The Bado classification of the Monteggia fracture is named after him.
Biography
- Born July 8, 1903 in Montevideo, Uruguay
- 1928 – Graduated as gold medal valedictorian from Universidad de la República, Montevideo
- 1928 – Worked at the military hospital for 2 years
- 1933 – 2 year scholarship, the Instituto Rizzoli in Bologna, Italy under Vittorio Putti (1880-1940)
- 1940 – Founded the Society of Trauma and Orthopaedics of Uruguay
- 1951 – Professor of orthopedics at Montevideo School of Medicine
- 1951 – First Chair of Orthopaedics and Traumatology at the School of Medicine, Montevideo
- 1962 – Publishes his eponym defining book: The Monteggia Lesion
- 1967 – Founded the Latin American Society of Orthopedics and Traumatology
- Died December 19, 1977 Montevideo, Uruguay
Observation is not enough; one must think; observation without thought is as dangerous as thought without observation
Bado JL
Medical Eponyms
Bado Classification (1958) of Monteggia fractures
Bado elaborated on the pathology, mechanics and management of the Monteggia fracture-dislocation first published in Spanish (1958), then in English (1962, 1967). Bado introduced the term Monteggia lesion and Monteggia equivalent injuries. He defined 4 injury patterns incorporating dislocation of the radial head associated with fractures at various levels of the ulna or with injuries at the wrist.
The Bado classification defines a group of traumatic ‘double bone‘ injuries having in common a ‘Monteggia lesion‘ (ulna fracture) with a dislocation of the radio-humero-ulna joint (radial head dislocation either anterior, lateral or posterior)
Since the dislocation of the radial head can be anterior, lateral or posterior, any dislocation found with an ulnar fracture constitutes the anatomic-clinical picture of the lesion discussed by Monteggia.
Keeping these considerations in mind, we shall be able to classify under the term ‘Monteggia lesion’ a group of traumatic lesions having in common a dislocation of the radio-humero-ulnar joint, associated with a fracture of the ulna at various levels or with lesions of the wrist. This concept is different from that described by Monteggia in 1814.
Bado 1967
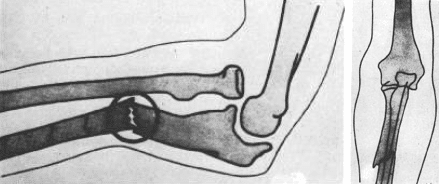
Type I: 60% of cases: Anterior radial head dislocation. Fracture ulna diaphysis with anterior angulation.

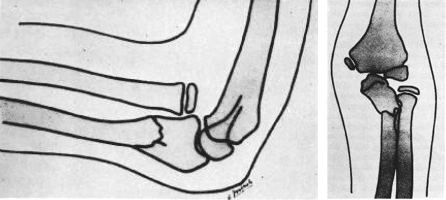
Type II: Fracture of middle or proximal third of the ulna shaft with posterior/posterolateral radial head dislocation (often fractured). 15% of cases. Trial of conservative management, open treatment required if ulna fracture does not reduce when radial head relocated.
Type III: Fracture of the proximal ulna metaphysis with lateral dislocation fo the radial head. 20% of cases. Occurs exclusively in children. Clinical deformity with increased transverse diameter of the elbow joint. Usually conservative treatment, risk of transient radial nerve paralysis post manipulation.

Type IV: Fracture of the middle or proximal third ulna AND anterior radial head dislocation AND a fracture of the middle third of the radial shaft. Infrequent, making up 5% of lesions and exclusive to adults. Open reduction fixation.
Key Medical Contributions
In 1954, Brazilian Flavio Kroeff-Pires (1917- ) first witnessed the technique of the Bier block demonstrated by one of Bado’s assistants. Bado had been using Bier’s method of intravenous regional anesthesia technique for many years, since visiting Bier’s medical school in Berlin during the 1920s. The technique had fallen out of favour but with the advancements of the cannula and safer local anesthetic agents, Kroeff-Pires re-ignited enthusiasm for IVRA.
Major Publications
- Bado JL. La lesion de Monteggia. Inter-Medica Sarandi, 1958: 328
- Bado JL. The Monteggia Lesion. 1962
- Bado JL. The Monteggia lesion. Clin Orthop Relat Res. 1967; 50: 71-86.
References
Biography
- José Luis Bado 1903–1977. J Bone Joint Surg Am. 1979 Jan;61(1):153-4.
- Mostofi SB. Who’s Who in Orthopedics. Springer. 2005: 17-19
- Biogtafía: José Luis Bado (1903-1977). Revista Colombiana de Ortopedia y Traumatología. 2006; 20: 18-20.
Eponymous terms
- Rehim SA, Maynard MA, Sebastin SJ, Chung KC. Monteggia fracture-dislocations: A Historical Review. J Hand Surg Am. 2014; 39(7): 1384–1394
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |