
![]()
Paracetamol…too much, too often?
aka Toxicology Conundrum 001
You are called by a doctor in a remote hospital asking for advice. The doctor is concerned about the risk of hepatotoxicity from repeated supratherapeutic ingestion (RSI) of paracetamol in the following patient:
A 46 year old male (75 kg) with 2 days of low back pain. He has self-medicated with a total of 10g of paracetamol over the past 48 hours:
6g over the first 24h followed by 4g over the past 24 hours.
He has no symptoms or signs of hepatoxicity at present.
Questions
Q1. Define paracetamol RSI.
Answer and interpretation
…the staggered dosing with therapeutic intent of paracetamol at >4g/day in adults or >60mg/kg/d in children. – Murray et al, 2007.
Q2. Is this patient at risk of hepatotoxicity due to RSI of paracetamol?
Answer and interpretation
Maybe…
Maybe not…
Further history is needed to determine if this patient falls into one of the 3 groups that require biochemical risk assessment:
Group 1
- Patients with a history of ingestion of 10g or >200mg/kg of paracetamol (whichever is lower) over a single 24 hour period.
- *The patient does not fall into this category.
Group 2
- Patients with a history of ingestion of 6g or >150mg/kg/24h of paracetamol (whichever is lower) for the preceding 48 hours or longer.
- *The patient does not fall into this category because he ingested 6g over a single 24 hour period followed by only 4g over the next 24 hours.
Group 3
- Patients susceptible to paracetamol due to other factors (such as alcoholism, isoniazid use, or prolonged fasting) with a history of ingestion of 4g or >100mg/kg of paracetamol (whichever is lower) over a single 24 hour period.
In this case the patient had no other risk factors for hepatoxicity and the patient was certain of the dose and timing of the ingestions of paracetamol. Thus no further investigation or management of potential hepatotoxicity was necessary.
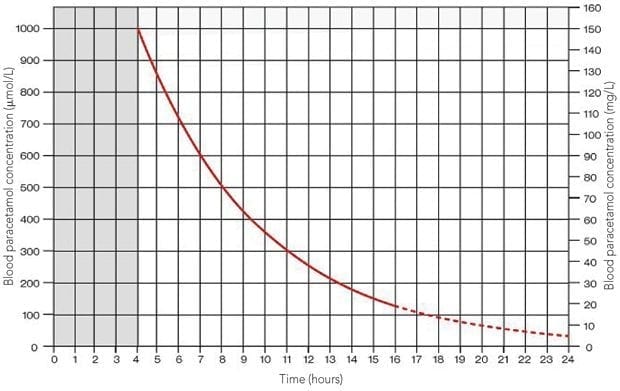
Discuss the use of the Rumack-Matthew or Prescott nomograms in this case.
Answer and interpretation
These nomograms are used to guide the treatment of acute paracetamol overdose and are not useful for the management of paracetamol RSI.
Note that a new simplified nomogram is now recommended for acute paracetamol ingestion.
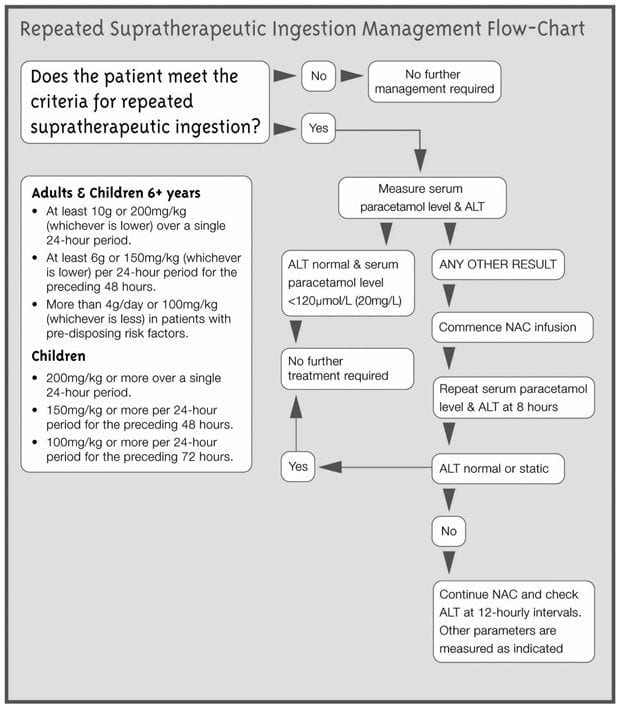
Q4. Describe the biochemical risk assessment of paracetamol RSI.
Answer and interpretation
Patients that fall into one of the three groups described in Q1 require biochemical risk assessment. This involves measurement of an untimed serum paracetamol level and a hepatic transaminase level (ALT or AST) at presentation to determine prognosis.
Good prognosis if:
paracetamol level <120 micromol/L (<20 mg/L)
AND
ALT or AST <50 IU/L
→ NO FURTHER INVESTIGATION OR TREATMENT REQUIRED
Higher risk if:
paracetamol level >120 micromol/L (>20 mg/L)
OR
ALT or AST >50 IU/L
→ TREATMENT WITH N-ACETYLCYSTEINE (NAC)
References
- Daly FFS, O’Malley GF, Heard K et al. Prospective evaluation of repeated supratherapeutic acetaminophen (paracetamol) ingestion. Annals of Emergency Medcine 2004; 44(4):393-398. PMID: 15459622
- Daly FFS, Fountain JS, Murray L, et al. Guidelines for the management of paracetamol poisoning in Australia and New Zealand — explanation and elaboration. Medical Journal of Australia 2008; 188 (5): 296-302. PMID: 18312195

CLINICAL CASES
Toxicology Conundrum
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
