
![]()
Rabies Vaccine
Indications and Role:
The UK recommends a vaccine called Rabipur or Rabies vaccine BP. These are both freeze dried chick embryo cells or human diploid cells retrospectively with inactivated virus. Once reconstituted they should be used within the hour.
Administration and dosing:
- Vaccines should be injected into the deltoid muscle for adults and children over 2 years. Anterolateral thigh is recommended for children younger than 2 years. Vaccines should not be injected into the gluteal region.
- Primary Pre-exposure:
- 3 doses of 1 ml (2.5 IU) intramuscularly on days 0, 7 and 28. The third dose can be given from day 21 if there is insufficient time before travel.
- Doses are injected into the upper arm or anterolateral thigh. Deep subcutaneous injections can be given to those with a bleeding disorder.
- ‘Off label’ dosing can be done via the intra-dermal which is just 0.1ml (0.25 IU) of vaccine with the same schedule. Rabipur and Verolab are the only two with proven safety. This has been done to reduce cost in many settings but should not be done in those taking chloroquine as this drug reduces the antibody response via this route.
- Boosters:
- Laboratory workers routinely working with rabies virus
- Primary course (3 doses of vaccine)
- Serology at 6 monthly intervals and booster if titre falls below 0.5 IU/ml
- Bat handlers, people who work with animals (vets) and health workers who work in rabies enzootic areas or working with patients with potential rabies.
- Primary course (3 doses of vaccine)
- Booster at 1 year
- Then booster every 3 to 5 years based on the results of serology
- Travellers to rabies enzootic areas
- Primary course (3 doses of vaccine)
- No serology
- Booster dose can be considered at 10 years post-primary course if travelling again to a high risk area.
- Laboratory workers routinely working with rabies virus
- Post-exposure prophylaxis (see also Rabies Immunoglobulin where required)
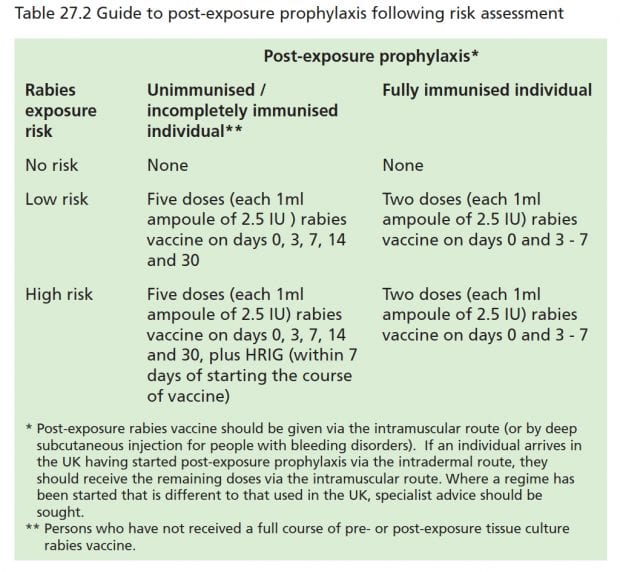
UK Recommendations:
Risk has also been categorised as low in those animals that are healthy and can be observed versus high risk in those that are wild, unwell or can not be observed.
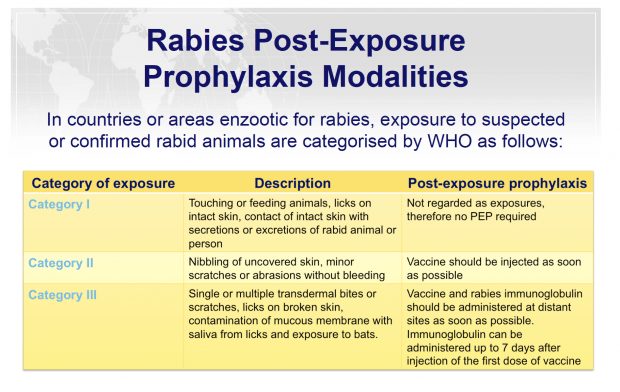
WHO Recommendations/Regimen:
- There are 3 WHO PEP schedules for the unimmunised:
- 5 dose intramuscular (1-1-1-1-1). One dose should be administered on days 0, 3, 7, 14 and 28
- The 2-1-1 regimen (2-0-1-0-1). Two doses are given on day 0 in the deltoid muscle, right and left arm. An additional dose is delivered on day 7 and on day 21.
- 2-site intradermal method, Rabipur and Verolab are the only two with proven safety (2-2-2-0-2). One dose of 0.1ml is given intradermally at two different lymphatic drainage sites, usually in the deltoid region on the left and right upper arm and supra scapular region on days 0, 3, 7 and 28.
- WHO schedule for the immunised, post exposure prophylaxis (2 schedules to chose):
- 1 dose intramuscularly or intradermally on days 0 and 3, or…
- “4-site” intradermal. This consists of 4 injections of 0.1ml equally distributed over left and right deltoids, thigh or supra scapular areas during a single visit.
Contraindications or complications and special populations:
- Pre-exposure rabies vaccine should not be given to those who have had a confirmed anaphylactic reaction to a previous dose or confirmed anaphylactic reaction to any component of the vaccine.
- There are no absolute contraindications to post-exposure prophylaxis with rabies vaccine.
- Safe in pregnancy, breast feeding and children
- Other vaccines can be given at the same time.
- Intradermal 0.1 ml pre-expousre vaccine regimen should not be used in those taking chloroquine.
- Individuals with immunosuppression and HIV infection (regardless of CD4 count) may not make a full antibody response and should have serological testing to determine if further dosing is needed especially once CD4 counts are above 200 or immunosuppression therapy has finished. Those who require post-exposure prophylaxis should be discussed with a specialist.
References
- The green book
- WHO guidelines (PEP prophylaxis – rabies 2014)
- Rabipur package leaflet information
- Rabies Vaccine BP leaflet information
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.