
![]()
Red Dust, dingoes, trauma and Sepsis
aka Postcards from the Edge 008
Guest post by Dr Chris Edwards recounts his time as a remote retrieval registrar based in Alice Springs
I’ve had the privilege to work as a Retrieval Registrar for the Alice Springs Hospital Retrieval Service in Central Australia for the last 6 months. How to describe it – words that spring to mind include:
- Challenging (unlike many other retrieval jobs, you often are intimately involved in the logistics planning)
- Satisfying (providing ICU level care to the most remote parts of Australia)
- Scary (providing ICU level care to the most remote parts of Australia!)
- Clinical character forming (Brown underpants occasionally needed)
- Interesting (When a potassium > 7 and severe rheumatic heart disease no longer turns your head)
- Scenic (people pay money to see Uluru from the air, I get paid)
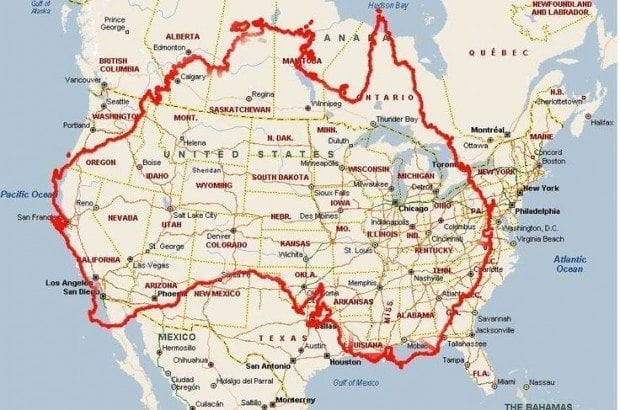
The Central Australian Retrieval service retrieves patients mainly by fixed wing aircraft over a catchment area of 1.6 million square km. We also perform inter-hospital transfers to Adelaide and Darwin (that’s 3.5 hours, one way, either way!) Let me try to put the sheer size of our catchment area and distance from our tertiary referral centres into perspective…
Here is Australia, our tertiary referral centres and our catchment area roughly outlined…

Here is a map of Australia overlaid on the USA
Here is a map of Australia overlaid on Europe

I think you get the idea – this is a huge catchment area! With one other small hospital in Tennant Creek, the rest of our primary retrievals are to remote health clinics, staffed by RANs (Remote Area Nurses).
In our primary retrieval we don’t have sub-specialty retrieval teams so we do it all, although we do occasionally take a paediatrician with us. Common conditions, mostly from our indigenous population but occasionally a grey nomad or overly adventurous backpacker, include:
- Trauma (usually penetrating or MVA)
- Sepsis (and sometimes overwhelming septic shock)
- Snake bites/stick bites
- Renal disease – Missed dialysis with APO and/or hyperkalaemia
- Threatened/established/imminent/delivered labours at term/pre-term (I mentioned the brown underpants right?)
- Paediatrics – URTIs, LRTIs, infected scabies, post-streptococcal glomerulonephritis
Mostly our patient population is young, less than 50 years old – I haven’t retrieved a single NOF fracture since I got here!
Then there’s the inter-hospital retrievals; Mostly to Adelaide, we take intubated patients on inotropes, trauma patients with chest drains and vacmat with spinal precautions, recently lysed STEMIs, including failed thrombolysis with ongoing arrhythmia for rescue PCI (52 shocks is my current record); I’ve even taken two patients so far with intracranial bleeds and extra-ventricular drains (first time I had even seen one).
Equipment and Staff
The plane we use is the Pilatus PC-12, a single-engine turboprop made by the Swiss. It has a cruising speed of approximately 500km/hr and a maximum service ceiling of 30,000ft with cabin pressurization of <8000ft. We operate with a single pilot and flight nurse. The passenger cabin is modified to carry two stretchers and 3 seats. The plane also comes with a hydraulic stretcher loader in the rear exit – maximum load of 182kg. The PC-12 is ideal for our environment – it can land on shorter strips and can be flown with only one pilot – keeping our take-off and landing weights down


On the plane, we carry the doctor’s bag, which contains central lines, arterial lines, fast trach intubating LMAs, rapid infusion catheters, EZ-IO, scalpels, bougies and other useful gear. We also have onboard a standalone intubation kit, cannulation kit, equipment for infusions, syringe drivers, pump sets, a full cold and warm drug box, an Oxylog 3000, a Zoll X-series monitor/defibrillator/pacer and of course the most important – coffee/tea bag. Additional equipment we can carry includes a maternity pack, trauma pack, neonatal pack, a vacmat, a humidicrib, paediatric ventilator, surfactant, a Sonosite M-Turbo and 2-4 units of packed RBCs.
Our Flight Nurses are the backbone of the clinical service. Trained in both critical care and midwifery they have a broad skill set and a lot of experience. They have invaluable clinical and logistical knowledge and when it comes to obstetric cases, my general approach is to ‘Remain Above The Navel’ and do what I’m told!

The Retrieval Doctors have a varied background – some are Rural and Remote Medicine trained, some are budding intensivists, but the majority are Emergency trainees. What we all need to have in common is the ability to be flexible and manage a difficult airway or an unstable patient on your own, supported by the FACEM in ED and Retrieval specialists.

Typical Day
No such thing as a typical day in this job. You might be heading to Adelaide with an ICU patient – if you do, that’s your whole day, because it’s a 3 hour one way trip. If you aren’t tasked to an inter-hospital transfer, at some point you will likely get an SMS from RFDS operations with a job. You check the email system and read the clinical information – then you call the clinic and speak to the RAN – get the latest details, suggest management or procedures and try to get a feel of how sick the patient is and what equipment you might need to bring. Then it’s a trip into the hospital if you aren’t already there, grabbing your gear and driving or taking a taxi out to the RFDS hanger.
Once there you load up the plane and head off. Most of our retrieval locations are within 1 hour’s flight from Alice Springs, with a few outliers like Elliot and Kiwirrkurra taking 2 hours. Flight time will usually include discussing the plan with your flight nurse and finding out any logistical challenges from your pilot (eg. Day strip only, weights permissible, pilot hours remaining).
Occasionally you may instead be tasked to go to a cattle station, roadhouse or the side of the road but in most cases you will be going to a clinic in a remote community. When you arrive, someone will meet you in a car to take you and your gear to the clinic. The clinics vary in size and equipment but most will have at least a small ‘Emergency’ room.

It’s hard to really describe accurately the first time you arrive at a remote community clinic. I remember being surprised by all the dogs (and the occasional donkey and camel) and the hurried advice from the flight nurse not to try and pet them. I remember the flies being everywhere (we carry mortein in the plane) and I remember the crowd that greeted us, largely children ages 5-12, mostly with crusty noses and curious smiles and scattered amongst them would be one or two proud elders. I even remember one time where I heard a commotion outside the clinic and popped my head outside to see several children beating a snake with a water bottle, right near where we would be loading the stretcher…
So, at the clinic, you assess your patient(s), perform therapy as necessary and package for transfer. It’s important in this job to not spend unnecessary time on the ground – because you, the plane and the crew are an important resource for a large area of Australia. Once you are ready, you load your patient into the ‘Troopy’.
The Toyota Land Cruiser 70 Troop Carrier, affectionally known as a ‘Troopy’ is the ubiquitous remote area 4wd transport all over the globe. In Central Australia they have been modified to carry one or two stretchers. Having ridden in the back of many of them now, I can definitely say that they are a bumpy ride, but they’re very reliable and spare parts are easy to get.
‘Troopy’ ambulance
After arriving at the plane, you load the patient, with or without an escort and head back to Alice Springs – unless another job comes through whilst you are in the air and nearby!


What is it like to live in Alice Springs
Alice Springs is great. Many of the junior hospital staff are on temporary placements as well – young trainees keen to explore the area. From social nights at the local pubs (Monte’s being the most popular), to bike rides, local hikes and camping trips. The mountain biking and trail running is truly world class with several professional class races held here and the rock climbing hides some real gems and capacity for endless new development.
Within 4 hours driving there are a host of great hiking and camping spots, many with large permanent water holes (some locals have canoes!)– Ormiston Gorge, Palm Valley, Kings Canyon and of course you can’t miss out on a trip to Uluru and you can take a plane there or drive.





Local events are varied and the peak season for events and tourists is in Winter. There’s the Finke Desert Race (which I was involved with as a medical officer at Finke), the Beanie Festival, Wide Open Spaces, the typically Territorian Henley on Todd, the Alice Springs Show, Territory Day (the one day of the year you get to buy and use fireworks) and the Camel Races.

Sounds exciting? Well I had a blast. It was a challenging job and I think it begins shaping you as a future consultant. The friends I made and the adventures I had were all great experiences. I urge anyone who might be interested to consider a 6 month rotation up here as a Retrieval Registrar – you’ll get a lot out of it!

BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |