
![]()
René-Jacques Croissant de Garengeot
René-Jacques Croissant de Garengeot (1688-1759) was a French surgeon
de Garengeot is best remembered for his description of the appendix within a femoral hernia sac, later named de Garengeot’s hernia. Born in Vitré, Brittany, into a family of surgeons, he studied under Jean-Louis Petit and rose to prominence as demonstrator of anatomy at the Jardin du Roi.
In 1731 he published his account of a 55-year-old woman with a painful groin swelling, in whom he found and reduced the appendix within a femoral hernia sac. This was the first recognition of this anatomical variant in a living patient. Later reports by Prudent Hévin (1785) and 19th-century surgeons extended knowledge of this condition, but Garengeot’s original observation remains foundational. Beyond hernia surgery, his 1720 Traité also devoted chapters to the management of lacrimal fistula, compiling contemporary approaches with probing, cautery, and trephining of the os unguis.
Garengeot’s name also endures in dentistry through the “clef de Garengeot”, a tooth-extracting instrument resembling a key. Though effective, it was notoriously traumatic, often removing fragments of bone along with the tooth. Despite criticism that his writings were more compilatory than original, Garengeot’s works spread surgical innovations across Europe and trained generations of practitioners.
Biographical Timeline
- Born July 30, 1688 in Vitré, Brittany.
- Early 1700s – Studied surgery in Paris, became a pupil of Georges Mareschal (1658–1736), first Surgeon-in-Ordinary to Louis XV.
- 1715 – Named demonstrator of anatomy at the Jardin du Roi.
- 1724 – Appointed Maître en chirurgie and received his surgical doctorate.
- 1731 – Published Traité des opérations de chirurgie (2e), in which he described finding the appendix within a femoral hernia sac (later termed de Garengeot’s hernia).
- 1740s – Served as Surgeon to the Hôpital de la Charité and member of the Académie Royale de Chirurgie.
- 1750s – Recognised as a leading Parisian surgeon and teacher; several instruments and procedures bear his refinements.
- Died on December 10, 1759 in Cologne, aged 71.
Medical Eponyms
De Garengeot’s Hernia (1731)
De Garengeot’s hernia refers to a femoral hernia containing the vermiform appendix, first described in 1731 by de Garengeot. To be distinguished from a femoral hernia containing Meckel’s diverticulum (Littre’s hernia) and appendix is found within an inguinal hernia (Amyand’s hernia)
Epidemiology: Extremely rare: incidence reported at 0.5–1% of femoral hernias, more recent reviews suggest up to 5%. Appendicitis within the hernia sac is even rarer: 0.08–0.5% of cases. De Garengeot’s Hernia occurs predominantly in elderly women, mirroring the demographics of femoral hernias. By 2025, ~400 cases have been reported worldwide.
Clinical Presentation: Usually presents as a painful, irreducible groin lump below the inguinal ligament, often mistaken for an incarcerated femoral or inguinal hernia. Systemic signs (fever, peritonitis) are often absent due to confinement of inflammation within the femoral sac.
Diagnosis and Management: Preoperative diagnosis is challenging; CT and ultrasound occasionally identify the appendix in the femoral canal. Surgical management combines appendicectomy and femoral hernia repair. Techniques: Lockwood (infra-inguinal), Lotheissen (trans-inguinal), McEvedy (high approach), or laparoscopy.
Historical Significance
1731 – Garengeot described a 55-year-old woman who developed a painful right groin swelling after lifting bread. At operation, a femoral hernia was found containing the appendix, which was reduced and the patient recovered.
Original
English
…Je trouvai dans le sac herniaire un petit corps allongé, adhérent, que je reconnus pour l’appendice du caecum. Je le remis dans le ventre, et après avoir pratiqué la cure ordinaire de la hernie, la malade se rétablit – de Garengeot, 1731
…I found in the hernial sac a small elongated body, adherent, which I recognised as the appendix of the caecum. I returned it into the abdomen, and after carrying out the usual cure of the hernia, the patient recovered – de Garengeot, 1731
1785 – Prudent Hévin (1715–1790) is often credited with performing the first appendicectomy for an appendix in a femoral hernia, usually dated to his article Des Hernies crurales (1785). In fact, Hévin did not excise an appendix. He reported another surgeon’s post-mortem findings of a perforated appendix within a femoral hernia sac. This is the earliest account of diseased appendix in a femoral hernia, but no appendicectomy was attempted.
Case 1 (Hévin’s operation): At La Charité, with M. Foubert, Hévin operated on a man with a strangulated femoral hernia. He found the intestine livid and adherent; he dilated the crural arch but left the adhesions intact. On the third day the intestine fistulised, discharging faecal matter, and eventually healed. This was not appendicitis, but a case of partial intestinal strangulation successfully managed.
Case 2 (Marigue’s autopsy, reported by Hévin): Hévin then recounted M. Marigue’s case of a patient who died after developing a large abscess in the thigh. At autopsy, Marigue found the vermiform appendix had slipped under the femoral ligament, perforated, and released faecal material into the tissues while solid matter continued per rectum. Hévin himself did not operate; he merely reported his colleague’s post-mortem finding.
Early 1800s – Tritschler (1806), Hesselbach (1814), Taramelli (1835), Javanelli (1836) provided case reports noting appendix/caecum within femoral hernia sacs.
1830-1840s – Merling (1836) describes a case operated by Tiedemann of a strangulated appendicular hernia; operation consisted of incision and drainage (I&D), not removal. Charyau (1837) and Cabaret (1842) both reported operating for appendix-containing femoral hernia, but again with I&D of abscess rather than appendectomy.
**Before the mid-to-late 19th century, surgical culture did not favour removal of the appendix. If suppuration occurred, incision and drainage was performed. The concept of formal appendectomy in this setting only emerged later in the 19th century, once appendicectomy became established practice for appendicitis.
2005 – The eponymous term was reinforced in English surgical literature by Akopian and Alexander
Many surgeons are familiar with Amyand hernia … However, few surgeons know of the contribution of René Jacques Croissant de Garengeot, an 18th century Parisian surgeon, to hernias. He is quoted in the literature as the first to describe the appendix in a femoral hernia sac… We also propose crediting Croissant de Garengeot by naming this condition after him. Although his full last name is Croissant de Garengeot, for convenience we suggest the simple diagnosis of ‘de Garengeot hernia.’
Akopian and Alexander, 2005
Key Medical Contributions
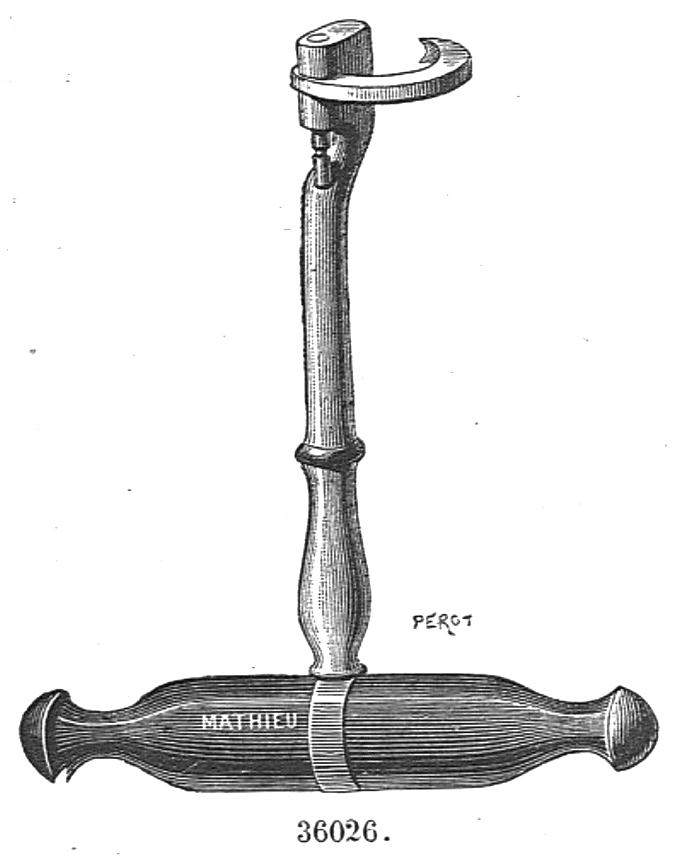
La Clef de Garengeot
In his 1723 Nouveau traité des instrumens de chirurgie les plus utiles, Garengeot introduced a brutal but influential dental extraction tool la clef de Garengeot (the Tooth Key). The instrument consisted of a stout handle with a shaft ending in a claw or hook. It was applied to a molar and rotated like turning a key in a lock, levering out the tooth. Its mechanical advantage was impressive, but the price was often the removal of fragments of the alveolar bone, producing severe trauma and lifelong complications.
Despite its risks, the clef de Garengeot became the standard tooth-extraction device of the 18th century, widely used across Europe and only supplanted later by more refined forceps. In dental history, Garengeot is remembered less for innovation in technique than for popularising this iconic instrument, which symbolises both the ingenuity and brutality of pre-anaesthetic surgery.
Lacrimal Surgery
In 1720, de Garengeot published his Traité des opérations de chirurgie, in which Chapters 37 and 38 were devoted to fistula lacrymalis. He built on the work of Jean-Louis Petit (1674–1750) and
Roland Paul Arnaud (1657–1723), cataloguing causes such as smallpox, scrofula, scurvy, venereal disease, trauma, and nasal polyps.
De Garengeot argued that stagnation of tears altered their properties, rendering them corrosive and leading to inflammation of the sac, rupture of vessels, and abscess formation. Treatments he described included compression, probing, incision, caustics, cautery, and even trephining the os unguis in cases of bony caries.
…les larmes, devenues acres et salées par leur stagnation, irritent le sac lacrymal et causent sa suppuration.
Although later critics considered his work derivative, his text helped codify contemporary management of lacrimal disease. He described a distinctive “bandage for a single eye”, 18 feet long, used by Petit to secure dressings.
Controversies
Name and naming convention
René-Jacques’s family name was Croissant, a dynasty of surgeons from Vitré. The addition “de Garengeot” derived from the family’s property “la terre de Garengcot” near Vitré, which conferred the style of a landholding sieur. In documents of the time he appears both as René-Jacques Croissant and René-Jacques Croissant de Garengeot.
French biographies often adopt the longer form Croissant de Garengeot, while some later sources abbreviated his name to “de Garengeot,” detaching it from its family context. This may have been reinforced by engravings and printed portraits that list him as “René-Jacques-Croissant DE GARENGEOT”
Birth Record
The archival evidence cited in Jarnouën de Villartay’s 19th-century biography includes the local parish register entry:
René, fils de Maistre Gilles Croissant et de Marguerite Ravenel, sa compagne, sieur de Garengcot, est né le 30 juillet 1688 et baptisé le 31 du dit mois.
Some later biographers, however, have repeated June 16, 1688 or marked the date uncertain. The primary record confirms July 30, 1688 as correct.
Major Publications
- De Garengeot RJC. Traité des opérations de chirurgie 1720 (Volume II) [English translation: A treatise of chirurgical operations 1723]
- De Garengeot RJC. Nouveau traité des instrumens de chirurgie. 1723
- De Garengeot RJC. Nouveau traité des instrumens de chirurgie les plus utiles. 1727 [Tome II] [Article VI “Du Pélican destiné pour arracher les dents”]
- De Garengeot RJC. Traité des opérations de chirurgie, fondé sur la mécanique des organes de l’homme, et sur la théorie et la pratique la plus autorisée. 1731, 2e [Hernia: 369–371]
- De Garengeot RJC. Traité des operations de chirurgie, fondé sur la mécanique des organes de l’homme, [et] sur la théorie [et] la pratique la plus autorisée. 1740
References
Biography
- Morand SF. Eloge de M. de Garengeot In: Opuscules de chirurgie. 1768: 69-81
- Jarnoüen de Villartay L. Essai de chirurgie historique. Garengeot, sa vie, son oeuvre, 1688-1759. Thèse de médecine de Paris. 1888-1889. N° 365.
- GARENGEOT (René-Jacques-Croissant de) In: Les médecins bretons du XVIe au XXe siècle : biographie et bibliographie 1900:2-4
- René-Jacques Croissant de Garengeot (1688–1759). Medical museum of NML.
Eponymous terms
- Hevin P. Des Hernies crurales In: Cours de pathologie et de thérapeutique chirurgicales. 1785: 407
- Tritschler FWG. Diss. sistens observationes in hernias praecipue intestini cocci, Tübingen. 1806
- Hesselbach FC. Neueste anatomisch-pathologische Untersuchungen über den Ursprung und das Fortschreiten der Leisten- und Schenkelbrüche, Würzburg. 1814
- Cabaret PJ. Hernie crurale de l’appendice cæcal, Journal de connaissances médico-chirurgicales, Paris, 1842; 10(1): 54–57
- Watson LF. Hernia of the vermiform appendix In: Hernia. 1924: 527
- Akopian G, Alexander M. De Garengeot hernia: appendicitis within a femoral hernia. Am Surg. 2005 Jun;71(6):526-7.
- Sharma H, Jha PK, Shekhawat NS, Memon B, Memon MA. De Garengeot hernia: an analysis of our experience. Hernia. 2007 Jun;11(3):235-8.
- Thomas B, Thomas M, McVay B, Chivate J. De Garengeot hernia. JSLS. 2009 Jul-Sep;13(3):455-7.
- Mizumoto R, Hendahewa R, Premaratne G. De Garengeot hernia-Use of a novel surgical approach and literature review. Int J Surg Case Rep. 2016;19:127-30.
- Guenther TM, Theodorou CM, Grace NL, Rinderknecht TN, Wiedeman JE. De Garengeot hernia: a systematic review. Surg Endosc. 2021 Feb;35(2):503-513.
- Yu PC, Wang LT, Chang CY, Tsai YC, Chong KH. De Garengeot Hernia, an acute appendicitis in the right femoral hernia canal, and successful management with transabdominal closure and appendectomy: a case Report. BMC Urol. 2024 Feb 16;24(1):41.
- Salawu A, Sarsam M, Butcher K. A case report and literature review of De Garengeot hernia. J Surg Case Rep. 2025 Jan 11;2025(1):rjae673.
- Ali MJ. Lacrimal History – Part 19: Doyens of Dacryology Series – René-Jacques Croissant de Garengeot (1688-1759) and His 1723 Treatise, ‘Traité des Operations de Chirurgie’. Semin Ophthalmol. 2025 Jun 20:1-4.
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |