
![]()
Richard Terry

Richard Barratt Terry (1914-1960) was an English Physician.
Trained at St Bartholomew’s hospital London. Specialist in liver disease, and liver biopsy at a time when there was much criticism of liver biopsy in some quarters, but, by his expert and reassuring handling of patients, Dr. Terry was able to impress many of his colleagues with the safety of his methods.
Remembered for his description of Terry’s nails in hepatic cirrhosis (1954); Red Half-moon nails in cardiac failure (1954) and modifications to instruments used in liver biopsy.
Biography
- Born on October 19, 1914
- 1932 – Completed school at Malvern College; entered medical school at King’s College, London
- 1933 – Transferred to St Bartholomew’s hospital to complete medical training
- 1938 – MBBS (Hons); House physician at St Bartholomew’s hospital
- 1939-1945 RAMC (TA) operating as a regimental and field ambulance medical officer in England and overseas
- 1945 – Supernumerary registrar at St Bartholomew’s hospital (MRCP and MD)
- 1946-1950 “Despite his long period of divorce from civilian medicine it was soon apparent that he was a man of unusual distinction, and he was properly rewarded by appointment as a medical chief assistant at Bart’s.” During this period he developed an interest in diseases of the liver; introduced an instrument to facilitate liver needle-biopsy; and published several valuable papers on this subject,
- 1950 – One year research Cook County Hospital, Chicago to broaden his experience of liver diseases
- 1952 – Consultant physician at the Dreadnought Seamen’s hospital
- 1954 – Emigrated to the United States with his wife and three young children to commence residency in Chicago
- 1955-1960 Worked in the Department of Medicine at Passavant Memorial Hospital and Cook County Hospital, Chicago. Teaching at Northwestern University Medical School, Chicago
- Died on October 3, 1960 (aged 45)
Medical Eponyms
Terry’s Nails (1954)
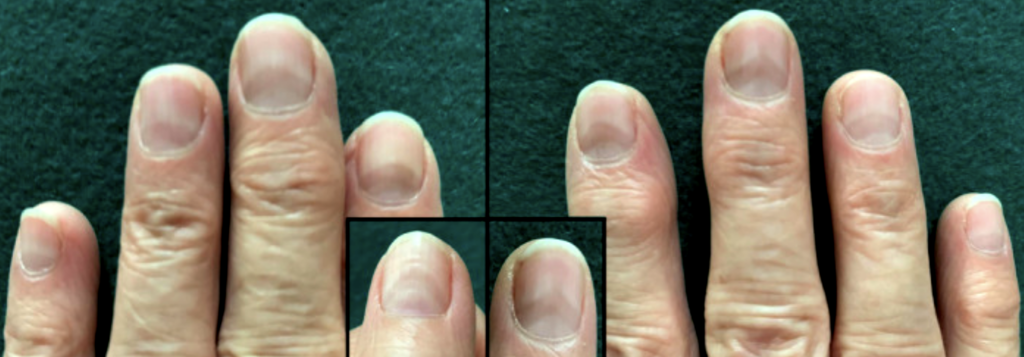
Terry’s nails are a type of apparent leukonychia, characterized by ground glass opacification of almost the entire nail, with a narrow band of normal, pink nail bed at the distal border, and often with obliteration of the lunula.
Fully developed white nails exhibit a ground-glass- like opacity of almost the entire nail bed. It extends from the base of the nail, where the lunula is indistinguishable, to within one or two millimetres of the distal border of the nail bed, leaving a distal zone of normal pink. The condition is bilaterally symmetrical, with a tendency to be more marked in the thumb and forefinger.
Terry 1954
The narrow pink/ brown segment (0.5 – 3 mm) of the distal border before the lunula indicates normal nail bed tissue. Opacity varies in degree and distribution: the most severe change is a proximal white nail with a dark band distally as shown below.

A: Distal thin pink-brown transverse band, 05-3mm wide, not obscured by venous congestion
B: white or light pink nail
C: lunula may or may not be present
Initially described by Richard Terry in 1954 in patients with cirrhosis (he found this sign in 82 of 100 cirrhotic patients) p < 0.01. This sign can also be manifested in other key systemic diseases such as chronic congestive heart failure (p <0.01), adult onset diabetes mellitus (p< 0.001) but also pulmonary tuberculosis, rheumatoid arthritis, convalescent viral hepatitis, disseminated sclerosis, renal failure and metastatic cancer. Terry’s nail is part of normal ageing and the above systemic diseases “age’ the nails quicker than normal.

Differential diagnosis for Terry’s nails includes half-and-half nails (Lindsay nails with only only about half of the proximal nail bed is opacified), Muehrcke lines (paired, white, transverse lines that typically spare the thumbnail), and true leukonychia totalis/partialis
Red Half-moon nails (Red lunulae) (1954)
The red lunula is characterized by replacement of the white lunula by red-pink or dusky erythematous discolouration. Terry originally described the red half-moons (red lunula) predominantly in patients with cardiac failure in 1954.
The half-moons of the nails, normally ground-glass in appearance, may become suffused or reddened. Such red half-moons have been observed in 23 patients, of whom 14 were suffering from cardiac failure…The remainder had disorders which were either primarily systemic, such as Hodgkin’s disease, or accompanied by systemic effects, such as hepatic cirrhosis. Red half-moons are apparently rare in healthy persons, and their detection may therefore be of some importance.
Terry 1954
Red lunula may be present on all or part of the lunulae, and may affect all digits. Aetiology is undetermined but red lunulae are most often associated with cardiac failure and autoimmune diseases such as rheumatoid arthritis, systemic lupus erythematosus, and alopecia areata. However multiple case reports exist with various disorders including cardiovascular, cutaneous, endocrine, gastrointestinal, haematologic, hepatic, infectious, neoplastic, and pulmonary.

2020 – Neri et al describe the nail changes of a 60 year old patient with a positive RT‐PCR nasopharyngeal swab confirmed SARS‐CoV‐2 infection. Two weeks following the onset of symptoms she developed a distally convex half‐moon‐shaped red band surrounding the distal margin of the lunula appeared on all fingernails.
Major Publications
- Terry R. Liver biopsy. St Bartholomews Hosp J. 1949; 53(10): 202‐204.
- Nicol CS, Terry RB. Late syphilis of the liver treated with penicillin. Br J Vener Dis. 1951; 27(1): 20‐22.
- Terry R. Risks of needle biopsy of the liver. Br Med J. 1952;1(4768):1102‐1105.
- Terry R. Liver biopsy. Br Med J 1953; 2: 1102
- Terry RB, Popper H. Boeck’s sarcoid of the liver. Proc Inst Med Chic. 1953;19(15):324‐325.
- Terry R. White nails in hepatic cirrhosis. Lancet. 1954; 266(6815): 757‐759. [Terry’s Nails]
- Terry R. Red half-moons in cardiac failure. Lancet. 1954; 267(6843): 842‐844
- Terry RB, Nixon RK. Instrument for splenic puncture. Lancet. 1954; 267(6840): 688‐689.
- Terry R. The onychodermal band in health and disease. Lancet. 1955; 268(6856): 179‐181.
- Terry R. Needle necropsy. J Clin Pathol. 1955;8(1):38‐41. doi:10.1136/jcp.8.1.38
- Terry RB, Gunnar RM. Primary miliary tuberculosis of the liver. J Am Med Assoc. 1957;164(2):150‐157.
- Terry RB. Incarcerated retroflexed gravid uterus; simple maneuver for its correction. Obstet Gynecol. 1959; 13(5): 630‐631
- Terry RB. Coupled hepatic pulsations in tricuspid incompetence; a new physical sign. Am Heart J. 1959; 57(1): 158‐159.
References
Biography
- Obituary: R. B. TERRY, M.D., M.R.C.P. Br Med J 1961; 1: 57
- Obituary: Dr R B Terry. Chicago Daily Tribune. Tuesday October 4 1960
- Richard Barratt Terry. Mendeley
{kind=link}
Eponymous terms
- Wilkerson MG, Wilkin JK. Red lunulae revisited: a clinical and histopathologic examination. J Am Acad Dermatol. 1989; 20(3): 453‐457.
- Cohen PR. Red lunulae: case report and literature review. J Am Acad Dermatol. 1992; 26(2 Pt 2): 292‐294
- Lindsley CB. Nail-bed lines in Kawasaki disease. Am J Dis Child. 1992 Jun;146(6):659-60.
- Wollina U, Barta U, Uhlemann C, Oelzner P. Lupus erythematosus-associated red lunula. J Am Acad Dermatol. 1999;41(3 Pt 1):419‐421.
- Chang P et al. Red lunula. Our Dermatol Online. 2013; 4(4): 555-556
- Neri I, Guglielmo A, Virdi A, Gaspari V, Starace M, Piraccini BM. The red half-moon nail sign: a novel manifestation of coronavirus infection. J Eur Acad Dermatol Venereol. 2020 Nov;34(11):e663-e665
- Cadogan M. Terry’s nails, Eponym A Day. instagram
- Wiesbauer F. Medical Treatment of Heart Failure. Medmastery
Eponym
the person behind the name

Graduated from Southampton Medical School in 2017 with BMBS. Working in Sir Charles Gairdner Hospital Emergency Department in Perth, Australia.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
The most complete biography of my father that I have ever seen! I was born in Chicago and he died three years later so I never knew him. Thank you so much for this treasure! Mark Terry