
![]()
Rigler sign
Rigler’s sign is a radiological indicator of pneumoperitoneum seen on supine abdominal X-ray. It appears when both sides of a bowel loop, the mucosal (inner) and serosal (outer) surfaces, are simultaneously outlined by gas. This occurs due to the presence of both intraluminal gas and free intraperitoneal air, rendering the normally invisible outer wall of the bowel visible.
Radiological Description
- Visualisation of both inner and outer walls of gas-filled bowel loops.
- Requires moderate volume of free intraperitoneal air to manifest.
- Best seen on supine abdominal films, particularly in neonates and critically ill patients unable to be imaged erect.
Clinical Relevance
- Seen in 14–32% of patients with gastrointestinal perforation.
- More commonly observed in gastric or colonic perforations.
- Pseudo-Rigler’s sign: may occur with abundant intraluminal gas, adjacent loop crowding, or mesenteric fat — not due to pneumoperitoneum.

History of the Rigler Sign
1915 – Hugo Popper, working under Prof. Mannaberg in Vienna, published “Die Diagnose der Darmperforation mit Hilfe der Röntgendurchleuchtung“. Popper’s early fluoroscopic observations represent one of the first published accounts of radiographically detected free intraperitoneal gas. He detailed how spontaneous pneumoperitoneum could be identified in patients with suspected gastrointestinal perforation by observing a sichelförmige Aufhellungszone (sickle-shaped lucency; Popper’s sign) beneath the diaphragm.
“Eine sichelförmige Aufhellungszone zwischen Zwerchfell und Leberkuppe… erlaubt die Diagnose der Perforation eines gasführenden Baucheingeweides mit voller Sicherheit.”
Popper 1915
A sickle-shaped lucency between the diaphragm and liver dome… allows the diagnosis of perforation of a gas-filled abdominal viscus with full certainty.
Popper described diagnostic significance in gastric and duodenal perforations as well as erect and decubitus positioning to confirm free air movement. He differentiated from Chilaiditi sign based on positional changes (disappearance when supine); lack of haustral patterning and brilliance and symmetry of the lucency.
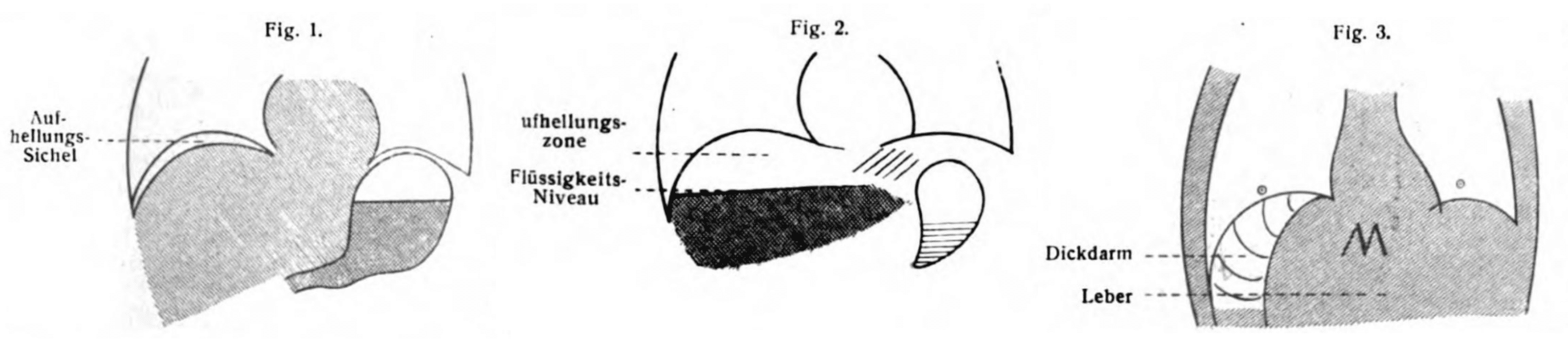
Fig. 2 – Decubitus position: Air-fluid level in the subhepatic space (Flüssigkeits-Niveau), emphasizing the value of positional change during fluoroscopy to confirm free peritoneal gas.
Fig. 3 – Chilaiditi mimic: Illustrates pseudopneumoperitoneum due to interposition of colon (Dickdarm) between the liver (Leber) and diaphragm. The presence of haustra and lack of positional shift help differentiate this from true free air. Popper, 1915
1924 – R. T. Vaughn and William A. Brams published The early recognition of acute perforation of gastric and duodenal ulcer by x-ray examination of spontaneous pneumoperitoneum. One of the earliest articles systematically describing the radiographic signs of free air due to gastrointestinal perforation. The authors emphasized the diagnostic value of radiographs even in the absence of classic upright or decubitus films.
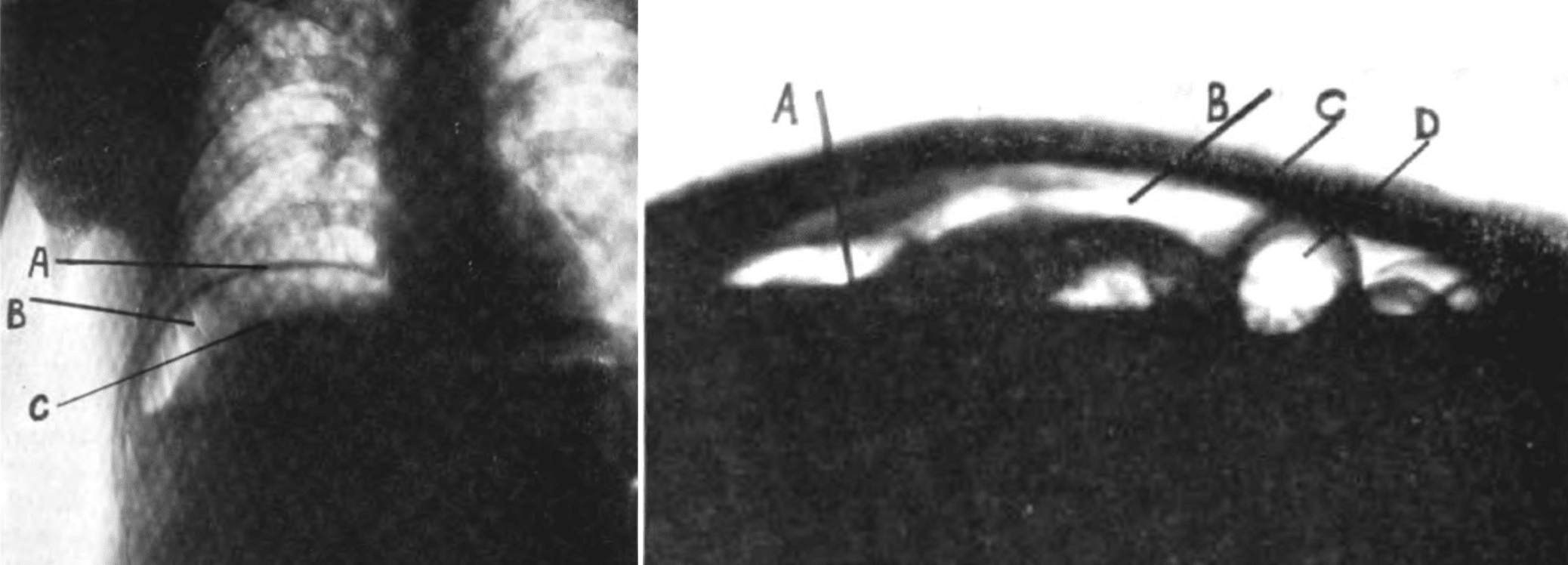
Left Fig.1. Erect X-ray A, dome of right diaphragm; B, free air under diaphragm; C, upper surface of liver.
Right Fig. 2. Supine decubitus X-ray A, level of fluid in free abdominal cavity; B, free air in abdominal cavity above the fluid level; C, anterior abdominal wall; D, loop of bowel containing air. Vaughn 1924
1941 – Leo George Rigler (1896-1979) described the pneumoperitoneum sign and emphasized that it would only be observed when large quantities of free gas were present.
A roentgenologic sign of pneumoperitoneum hitherto not reported or clearly defined is described. It consists of the demonstration of the outer as well as the inner bowel wall due to the accumulation of gas between the loops of bowel. It is of value because it can be observed in roentgenograms of the abdomen made in the supine position.
This sign may be the first evidence of the presence of pneumoperitoneum in cases in which such a condition is entirely unsuspected. Routine roentgenograms of the abdomen should be made at frequent intervals in all cases of obstruction of the gastro-intestinal tract which are being treated conservatively. Such films should always be examined for evidences of pneumoperitoneum because of the possibility of supervention of perforation without obvious clinical signs.
Rigler, Radiology 1941
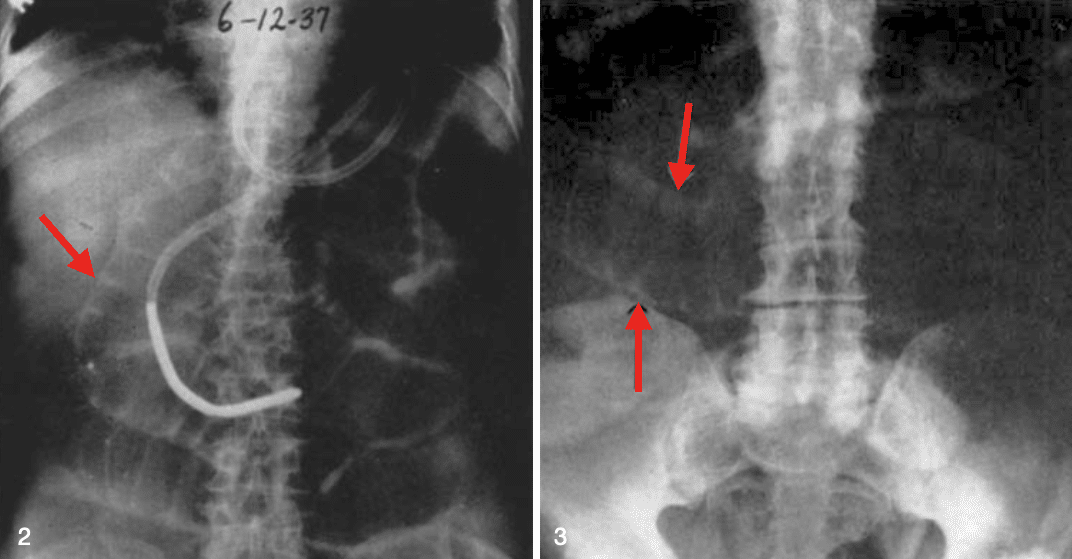
Fig. 3. Case of perforation of the colon with pneumoperitoneum; roentgenogram of abdomen, supine position. Note the distended loops of small bowel, both their inner and outer contours (arrows) being readily visible. Rigler 1941
1960 – Roscoe E. Miller (1918-1984) of the Indiana University School of Medicine described the “air dome” sign in a series of infants with gastric, duodenal, or colonic perforation. This was based on a large review of supine radiographs from patients too ill for erect imaging.
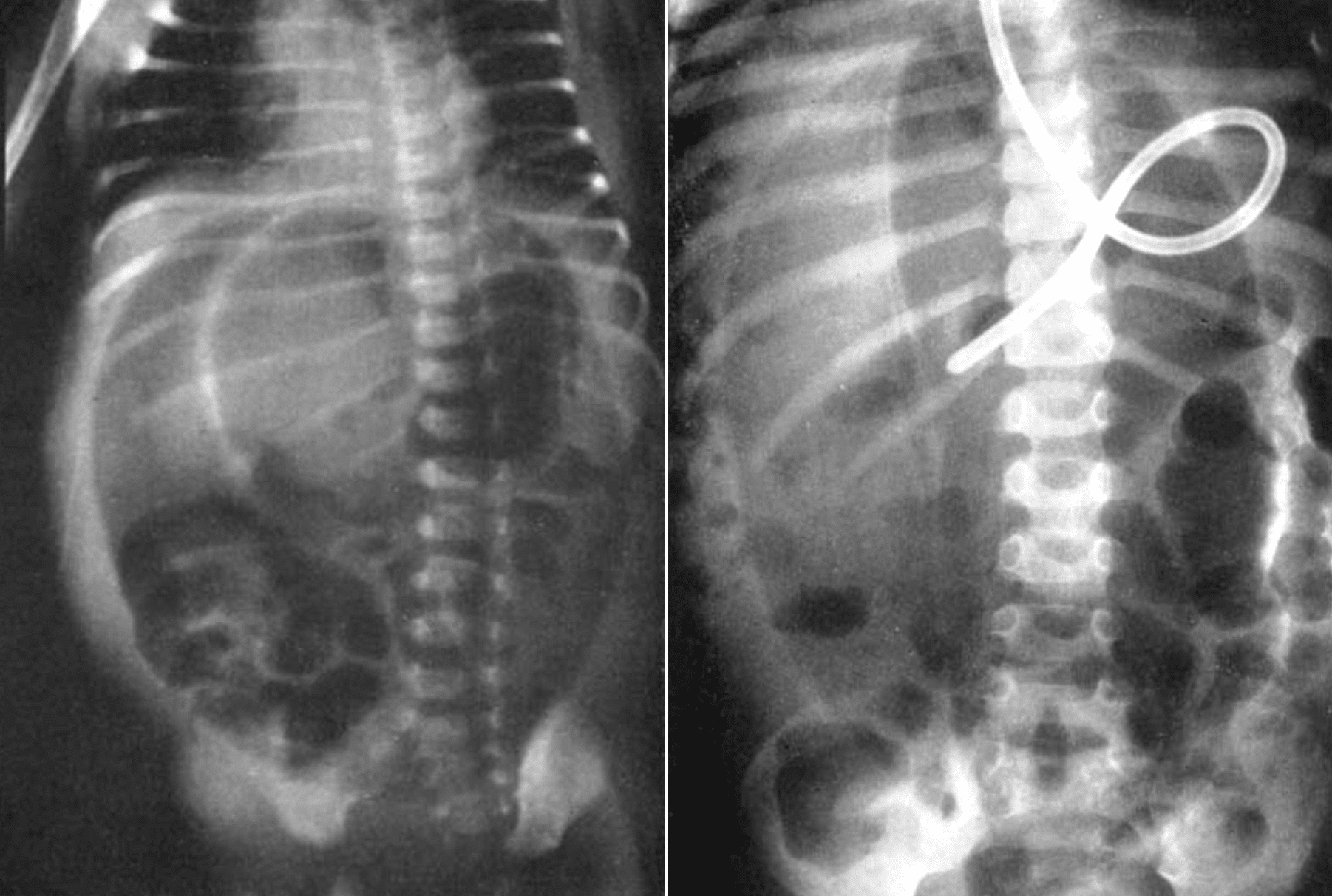
Figure 2: Supine radiograph in a 4-year-old showing similar air dome, with confirmed duodenal perforation at autopsy. Miller 1960
Miller’s sign emphasised the early and specific recognition of free air in neonates using only supine films, significantly aiding diagnosis when other signs were absent or patients were non-ambulatory.
Confirmatory upright films may be taken, but it is unnecessary if the “air dome” sign is seen on the supine view. The “football” or “air dome” sign is pathognomonic and leads to early diagnosis and surgical intervention…The characteristic oval line of the “air dome” divided by the streak of the falciform ligament is pathognomonic.
Miller, 1960
1973 – Charles I. Weiner et al presented three cases demonstrating a further sign of pneumoperitoneum – the inverted V sign. Free air outlining the lateral umbilical ligaments makes these structures visible in the lower abdomen, forming an “inverted V” as they course inferiorly and laterally from the umbilicus. The ligaments contain the umbilical arterial remnants and may be unilaterally or fractionally visualized.
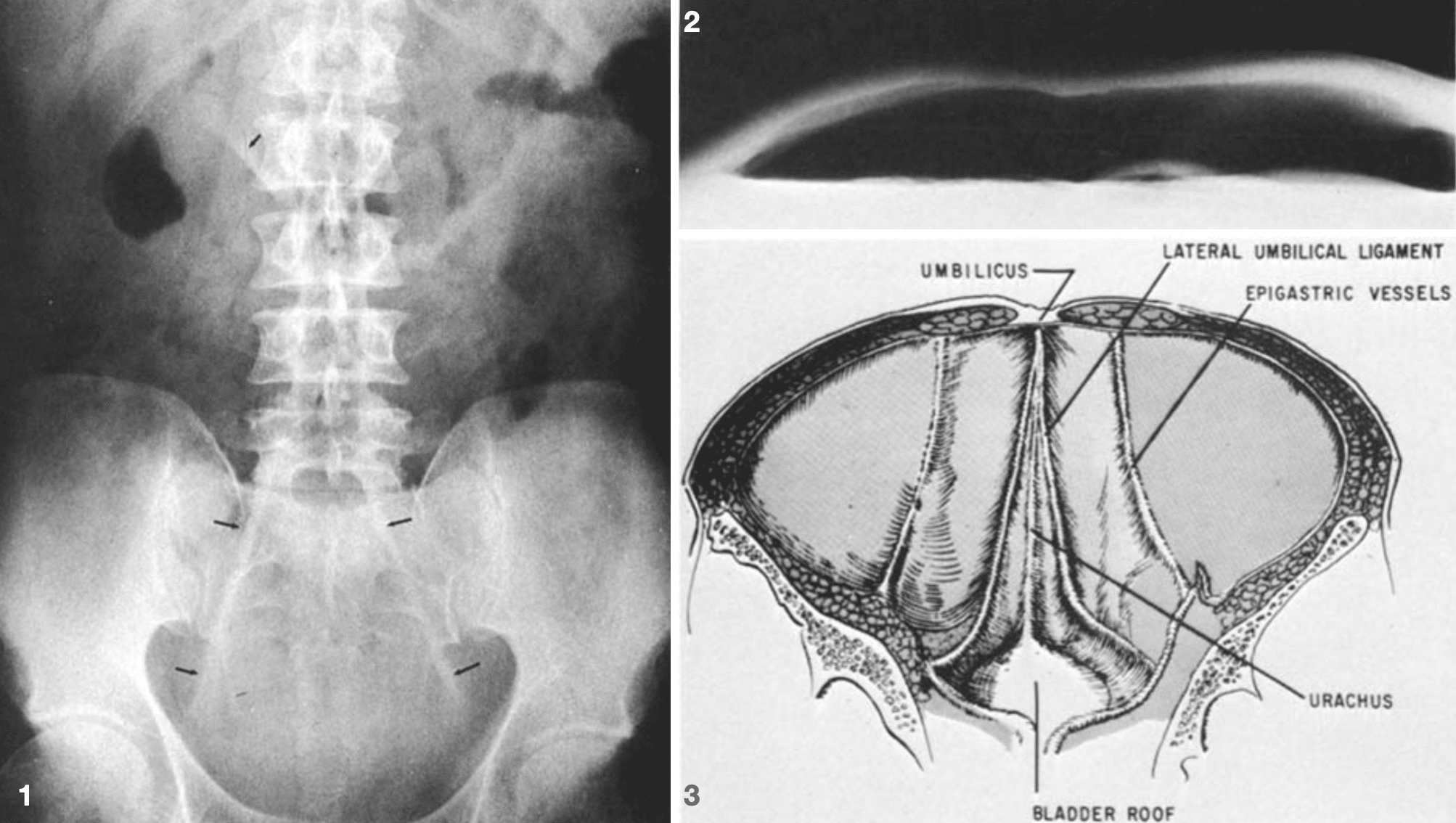
Fig. 1. Supine AXR showing lateral umbilical ligaments (lower arrows) diverging from the umbilicus. Free air also made the falciform ligament visible (upper arrow).
Fig. 2. Cross-table lateral AXR demonstrating massive pneumoperitoneum.
Fig. 3. Illustration of inner surface of lower anterior abdominal wall. Weiner 1973
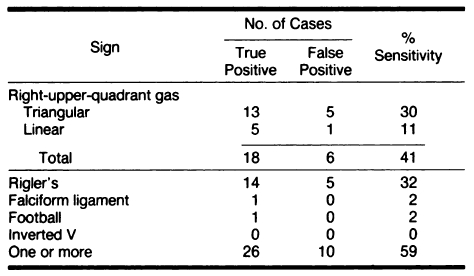
1991 – Marc S. Levine et al compared multiple supine signs (Rigler’s, falciform ligament, football, inverted V, and RUQ gas signs) in detecting pneumoperitoneum. Reinforced that while some signs like Rigler’s remain highly specific, no single sign is universally sensitive.
Pseudo-Rigler sign
Form of pseudopneumoperitoneum, and mimic of the classic Rigler sign, which can be encountered on normal abdominal X-rays.
Caused by omental / mesenteric fat; oral contrast media outlining the bowel loops; or overlapping gas-filled bowel loops making the wall contours appear more prominent.
In such cases further examination with erect or lateral decubitus views, or CT are required to rule in or out the presence of free gas.
Associated Persons
- Leo George Rigler (1896-1979)
- Roscoe E. Miller (1918-1984)
Alternative names
- Double-wall signs: Rigler’s, Double-lumen, Bas-relief
- Shape-based signs: Football sign, Inverted V sign, Air dome sign
References
Original references
- Popper H. Die Diagnose der Darmperforation mit Hilfe der Röntgendurchleuchtung. Dtsch Med Wochenschr 1915; 41(35): 1034-1036 [Popper’s sign]
- Vaughn RT, Brams WA. The early recognition of acute perforation of gastric and duodenal ulcer by x-ray examination of spontaneous pneumoperitoneum. Surg Gynecol Obstet 1924; 39: 610-617
- Rigler LG. Spontaneous pneumoperitoneum: a roentgenologic sign found in the supine position. Radiology 1941; 37: 604–607 [Rigler’s sign]
- Miller RE. Perforated viscus in infants: a new roentgen sign. Radiology. 1960 Jan;74:65-7. [Air Dome or Football sign]
- Weiner CI, Diaconis JN, Dennis JM. The “inverted V”: a new sign of pneumoperitoneum. Radiology. 1973 Apr;107(1):47-8. [inverted V sign]
Review articles
- Miller RE, Nelson SW. The roentgenologic demonstration of tiny amounts of free intraperitoneal gas: experimental and clinical studies. AJR 1971; 112: 574-585
- Bray JF. The “inverted V” sign of pneumoperitoneum. Radiology. 1984 Apr;151(1):45-6.
- Levine MS, Scheiner JD, Rubesin SE, Laufer I, Herlinger H. Diagnosis of pneumoperitoneum on supine abdominal radiographs. AJR Am J Roentgenol 1991; 156(4): 731–735
- Williams N, Everson NW. Radiological confirmation of intraperitoneal free gas. Ann R Coll Surg Engl. 1997 Jan;79(1):8-12
- Ly JQ. The Rigler sign. Radiology. 2003 Sep;228(3):706-7.
- Lewicki AM. The Rigler sign and Leo G. Rigler. Radiology. 2004 Oct;233(1): 7-12
- Daya S, Mahomed N, Andronikou S. Rigler’s sign and the football sign. South African Journal of Radiology. 2012; 16(4): a263
- Indiran V, Sivakumar V. Rigler sign. Abdominal Radiology, 2017; 42(10): 2588–2588
- Al Kabbani A. Rigler sign (bowel). Radiopaedia
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |