
![]()
Roman Breastplate
aka Trauma Tribulation 005
A 35 year-old man was involved in a house fire and sustained extensive severe burns, particularly affecting his trunk and upper limbs. The patient is shown undergoing a procedure:
Questions
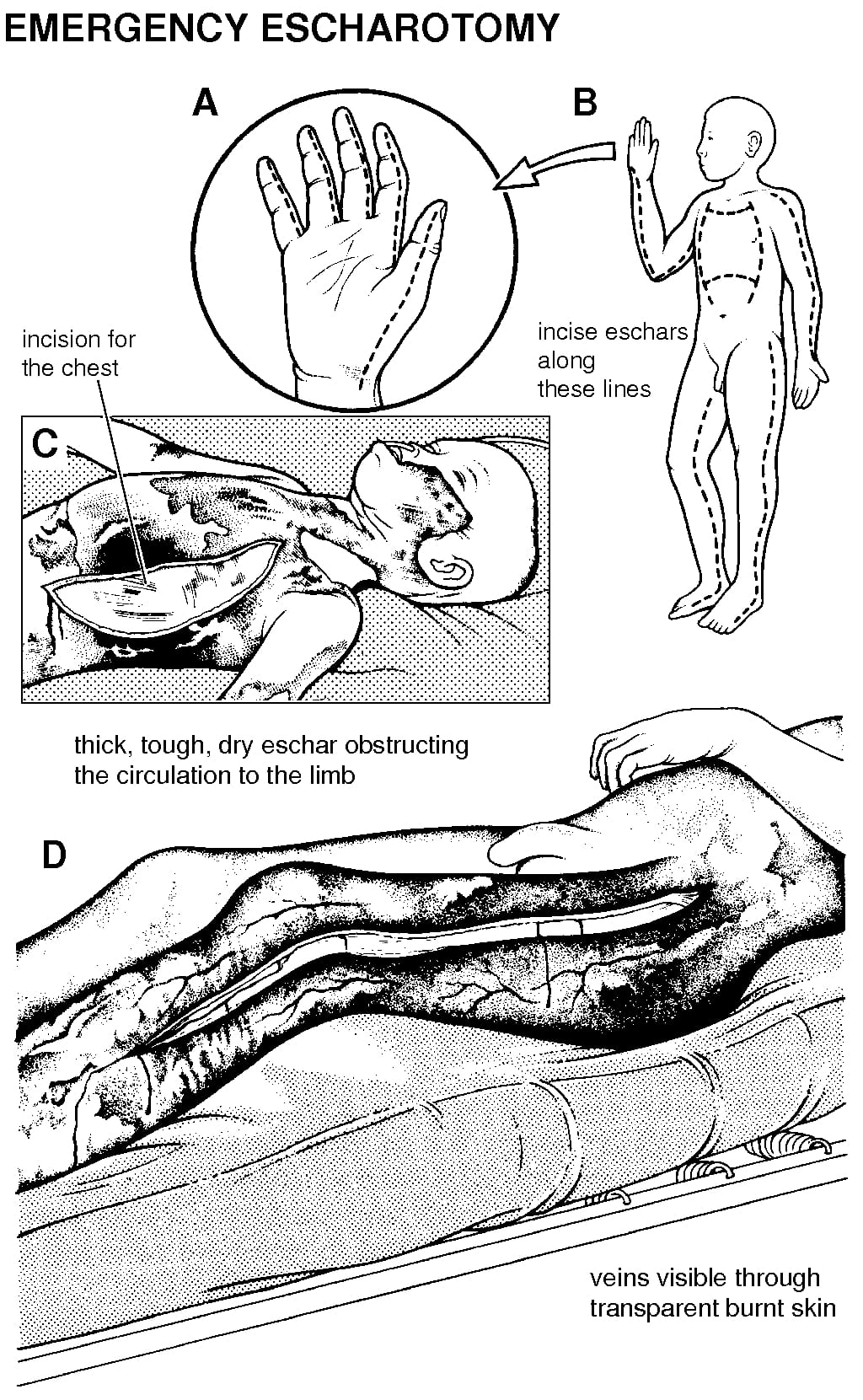
Q1. Describe the appearance of the skin on the patient’s chest?
Answer and interpretation
The skin has been severely burned. It has a leathery appearance consistent with the coagulated dead skin of a full thickness burn.
This is called eschar.
In a full thickness burn epidermis and dermis are destroyed, and the burn may penetrate more deeply into underlying structures. The sensory nerves in the dermis are destroyed, so pinprick sensation will be absent.
Q2. What procedure is being performed?
Answer and interpretation
Escharotomy
Although this rarely needs to be performed in the ED, studies have shown that a reluctance to perform escharotomies means nearly half of all pediatric burns patients have inadequately released burns prior to arrival at a tertiary burns centre.
Q3. When should this procedure be performed?
Answer and interpretation
Once eschar formation occurs the skin loses its expansibility and becomes restrictive. Progressive edema due to capillary leak, especially following fluid resuscitation, can have dire consequences. An escharotomy may be needed to release the burn and allow expansion.
Indications for escharotomy include:
- circumferential burns of the chestthat increase chest wall rigidity and impair ventilation (e.g. increased peak airway pressures in the ventilated patient).
- children may have predominantly diaphragmatic breathing so an escharotomy may be required even if the burn is limited to the anterior chest and abdomen (non-circumferential).
- constrictive circumferential neck burns that threaten the airway.
- circumferential burns of the extremitiesresulting in circulatory embarrassment/ compartment syndrome.
- The escharotomy should be permed once there is evidence of decreased circulation to the extremity, but before there pulses are lost (e.g. using doppler ultrasound, or SaO2<90% on pulse oximetry of the affected limb)).
Q4. Describe how the procedure is performed.
Answer and interpretation
Preparation
The procedure should be performed in a sterile fashion. It usually takes place in an operating room, but it can be performed in the ED or the field in emergency situations.
Use a surgical marker to define the intended lines of incision with the limbs in anatomical position. The forearms will need to be supinated.
Anesthesia
Anesthesia is not essential as the eschar is insensate. Local anesthetic may be infiltrated at the edge of the burn where incisions will be extended into normal skin. Nevertheless, the patients are often intubated and sedated due to the severity of the burns or associated trauma.
Hemorrhage
Blood loss can be severe – have artery forceps and ties, diathermy or topical hemostatics (such as calcium alginate) at the ready.
Incisions
The burned skin is incised down to the subcutaneous fat with a scalpel or cutting diathermy. They should be deep enough for obvious separation of the wound edges to occur. If in doubt, run a finger along the incision to detect any residual restrictive defects. The incisions should extend into normal skin by up to 1 cm.
- Trunk
- Longitudinal incisions along the anterior axillary lines to the costal margins, or upper abdomen if also burnt.
- These longitudinal incisions are connected by convex upwards transverse incisions below the clavicles across the upper chest, and across the upper abdomen.
- Limbs
- Longitudinal incisions along the mid-axial lines between the extensor and flexoral surfaces. Incisions along the flexural creases of joints are avoided.
- Lower limbs: The medial incision should pass anterior to the medial malleolus and avoid the long saphenous vein and saphenous nerve. Lateral incisions are made in the midlateral line, avoiding the common peroneal nerve at the neck of the fibula.
- Upper limbs: The medial incision should pass anterior to the medial epicondyle to avoid the ulnar nerve at the elbow. On the medial aspect of the hand the incision may progress as far as the base of the little finger. On the lateral aspect of the hand the incision can progress to the proximal phalanx of the thumb. Sometimes an incision along one side of a limb is sufficient to preserve circulation.
- Neck
- usually performed laterally and posteriorly to decrease risk of damage to the carotid arteries and jugular veins.
- Penis
- midlateral incisions to avoid the dorsal vein.
Q5. Which vulnerable areas require extreme caution?
Answer and interpretation
Structures immediately beneath the skin – nerves and vessels – are most vulnerable to damage during an escharotomy.
Structures particularly at risk of damage include:
- the ulnar nerve (incision should pass in front of the medial epicondyle)
- the peroneal nerve near (incision should not pass over the neck of fibula)
- the posterior tibial arteries and nerve and the long saphenous vein and saphenous nerve (incision should pass anterior to the medial malleolus)
Transverse incisions on the limbs should be avoided.
Q6. What are the complications of escharotomy, including when it is inadequately performed?
Answer and interpretation
Escharotomy may be complicated by:
- bleeding
- infection
- damage to underlying structures
Inadequate escharotomy may be complicated by:
- local effects: muscle necrosis, compressive neuropathy, amputation, inadequate ventilation, airway obstruction, abdominal compartment syndrome
- systemic effects: rhabdomyolysis (renal impairment, hyperkalemia, metabolic acidosis)

CLINICAL CASES
Trauma Tribulation
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
