
![]()
Splat! A vomiting infant
aka Pediatric Perplexity 006
A 6 week old baby boy (born at 36 weeks gestation) has seen a multiple doctors over the past 2 weeks because of vomiting. He has been started on omeprazole and thickened feeds to treat a presumptive diagnosis of reflux.
His parents are concerned as he remains unwell. They have brought him to your emergency department for further review. His vomiting is worse and occurs after every feed. His nappies are much less wet than usual, he is listless and he has had ~500g of weight loss over the last week.
Questions
Q1. What are the important differentials to consider in infants with vomiting?
Answer and interpretation
According to Rosen’s, the main causes of vomiting in infancy are:
- Mechanical causes — gastroesophageal reflux disease, pyloric stenosis, malrotation with midgut volvulus, intussusception, incarcerated hernia, and tracheoesophageal fistula
- Inflammatory and infectious causes — necrotizing enterocolitis, gastroenteritis, sepsis, meningtis, pneumonia, and otits media
- Genitourinary causes — UTI
- CNS causes — hydrocephalus, intracranial hemorrhage, and intracranial tumour
- Metabolic — DKA, congenital adrenal hyperplasia, organic acidurias, amino acidopathies, urea cycle disorders, and FFA oxidation disorders
- Other — occult trauma or non-accidental injury, toxic ingestion or envenoming (e.g. redback spider), and Munchausen’s by proxy
Also, I should mention a useful mnemonic (I think I picked it up from EM:RAP) for the major differentials in any really sick infant:
SICCC-FIT
Sepsis, IEMs, Congenital heart disease, CNS disorders, Congenital adrenal hypoplasia, Feeding problems, Intestinal disorders and Toxins.
His mother describes the vomitus as resembling ‘curdled milk’.
Q2. What are the possible underlying causes of this condition?
Answer and interpretation
The major causes of non-bilious vomiting in infants are:
- Pyloric stenosis
- GORD
- Infection (especially UTI and gastroenteritis)
While you assess the baby, he vomits. Splat! You are now wearing it. The word ‘projectile’ springs to mind.
Q3. What is the likely diagnosis?
Answer and interpretation
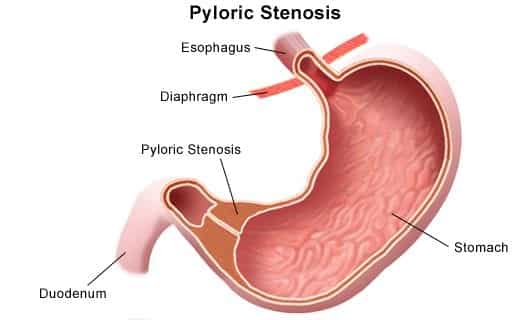
Pyloric stenosis aka HPS (hypertrophic pyloric stenosis)
This is a condition characterised by narrowing of the pylorus occurring in early infancy, ultimately causing gastric outlet obstruction. It affects about 1 in 250 live births in North America and Western Europe and is of uncertain etiology. Pyloric stenosis is uncommon in many other parts of the world.
The condition can be difficult to diagnosis clinically and requires a high index of suspicion.
Q4. What are the risk factors for this condition?
Answer and interpretation
Risk factors for pyloric stenosis include:
- Male (RR=4)
- First born
- Caucasian
- familial tendency (especially maternal)
Q5. On taking a history, what features would be consistent with this diagnosis?
Answer and interpretation
Typical features on history include:
- Presentation at age 2-12 weeks (regardless of prematurity)
- Projectile vomiting
- especially during or after feeding
- nonbilious (10% blood stained)
- progressively more forceful
- Failure to thrive
- Ravenously hungry after feeding
- Diarrhoea not usually present
Q6. What features on examination must be assessed when considering this diagnosis?
Answer and interpretation
Assess the following on examination:
- dehydration status
- weight loss (plot growth chart)
- jaundice (1-2%)
- Visible gastric peristalsis (from LUQ to RUQ) due to gastric obstruction
- palpable olive-like tumor in RUQ
- especially when feeding or when prone feel from the left-side flex the child’s hips to relax the abdominal musculature. If required, administer oral sucrose to stop crying.wait a few minutes! (some experts advise up to 20 minutes…)sensitivity may be as low as 25% (pediatric surgeons are better)
- marasmus may result

A venous gas is obtained:
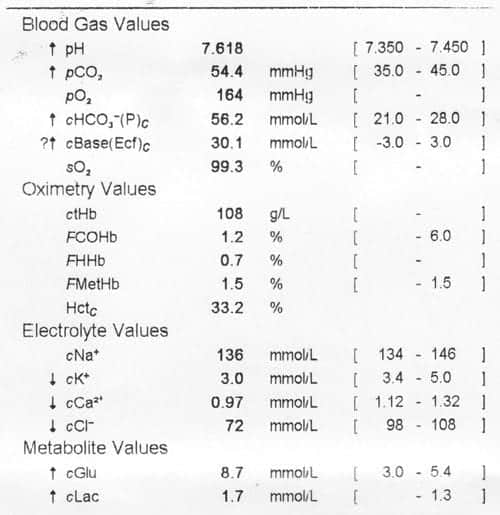
Q7. Describe the findings on the venous blood gas?
Answer and interpretation
The key findings on the venous gas are:
- Severe metabolic alkalosis with partial respiratory compensation
- Hypokalemia
- Hypochloremia
Q8. Is the venous gas consistent with the pathophysiology of the suspected diagnosis?
Answer and interpretation
Yes
The pylorus is normal at birth. There is progressive hypertrophy of the pyloric muscle resulting in gastric outlet obstruction. This manifests as vomiting and results in the loss of HCl and hypovolemia. The kidneys attempt to compensate for the loss of acid by retaining protons in exchange for potassium.
Thus the characteristic metabolic profile of pyloric stenosis is hypochloremic hypokalemic metabolic alkalosis.
Q9. What is the key investigation for clinching the diagnosis, and what other investigations would you perform?
Answer and interpretation
If detected, palpation of the ‘olive’ may be all that is needed — it’s positive predictive value is reported to be as high as 99%. If not:
Pyloric stenosis is best diagnosed using ultrasound, which is ~99% sensitive and specific if performed by an experienced ultrasonographer.

Other useful investigations include:
Bedside tests
- Glucose and VBG (hypochloremic hypokalemic metabolic alkalosis)
Laboratory tests
- UEC, FBC, Bilirubin/ LFTs
Imaging
- Ultrasound, especially if a mass not clinically palpable (e.g. due to abdominal distention)
- Upper GI contrast XR is an alternative:
- string sign — thin contrast leak
- modified double bubble sign — enlarged body and pylorus
- similar sensitivity and specificity to ultrasound
- useful for investigating reflux or if ultrasound is not available
Q10. Describe your approach to the management of this condition.
Answer and interpretation
Fluid resuscitation
- 10-20ml/kg boluses of 0.9% NaCl, for moderate/severe dehydration
Fluid replacement and maintenance
- Use 0.45% saline with 5% dextrose
- Calculate fluid deficit based on known weight when well
- Monitor q4-6h with UEC and VBG and adjust accordingly
- Aim to correct fluid and electrolyte status over 24-48h
- Add potassium once passing urine e.g. 20 mmol KCl/L of replacement fluid
Stop oral feeds
- Place NGT if ongoing vomiting
- feeding is usually restarted 6h post-op
Surgery — Ramstedt pyloromyotomy
- Performed following rehydration and correction of bicarbonate (hypoventilation risk in OT)
- most infants discharged 3 days post-op, but some will vomit for several days afterwards
- 1-2% of cases develop restenosis
- a laparoscopic approach may be preferred (lower rates of wound complications)
References
- Sharwood E. Pyloric Stenosis. DFTB
- Taghavi, K., Powell, E., Patel, B., & McBride, C. A. (2017). The treatment of pyloric stenosis: Evolution in practice. Journal of Paediatrics and Child Health. 2017;53(11):1105–1110.
- Aspelund G, Langer JC. Current management of hypertrophic pyloric stenosis. Semin Pediatr Surg. 2007 Feb;16(1):27-33. PMID: 17210480.
- MacMahon B. The continuing enigma of pyloric stenosis of infancy: a review. Epidemiology. 2006 Mar;17(2):195-201. PMID: 16477261.
- RCH Melbourne CPG. Pyloric stenosis.
- Sola JE, Neville HL. Laparoscopic vs open pyloromyotomy: a systematic review and meta-analysis. J Pediatr Surg. 2009 Aug;44(8):1631-7. PMID: 19635317

CLINICAL CASES
Paediatric Perplexity
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
