
![]()
Tetanus MCQ
Tetanus MCQ
Q1. Which of the following is true for the tetanus vaccine?
A. Every traveller should be up to date.
B. No one should have more than 6 shots in their lifetime.
C. Reactions are less likely to occur the more you have.
D. A tetanus vaccine should only be given to highly contaminated wounds regardless or vaccine status.
Answer and interpretation
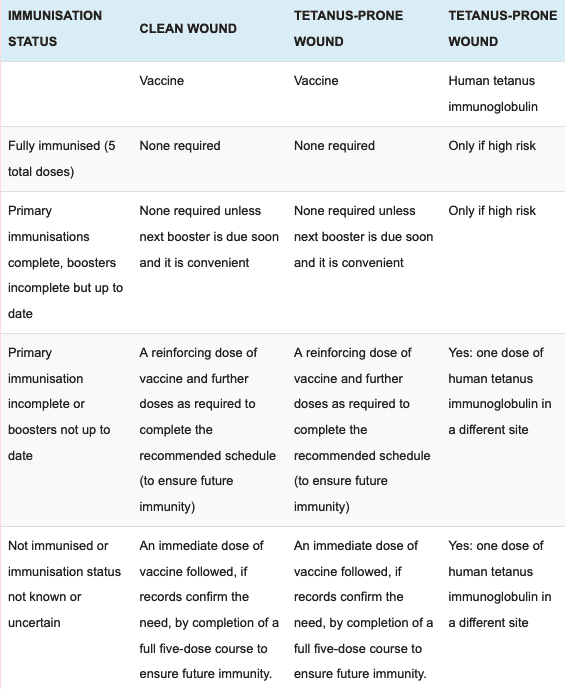
A, Tetanus should always be considered and given if required. About 25% of travellers are not up to date. UK advice is that 5 vaccines in a lifetime should be protective but countries differ and it is safe to have more, although the risk of a reaction increases slightly. In addition if you have a wound at risk then a booster can be given, see table below:
Q2. Regarding tetanus quick sticks (TQS)?
A. They take 1 hour to read.
B. If the test is positive, the patient has contracted tetanus.
C. They are 100% specific.
D. They are 80% sensitive for titres of 0.01 IU/ml.
Answer and interpretation
C, TQS take 10 mins to read and are 100% specific for tetanus antibodies. If the test is positive you can assume the patient has protection against tetanus for at least 5 years. Sensitivity is 55% for titres of 0.01 IU/ml but 100% if titres >0.5 IU/ml, which is 5x greater than the accepted protective limit of 0.1 IU/ml.
Q3. Regarding tetanus immunisation?
A. Local reactions can be as high as 10%.
B. It is not necessary for the over 75 year olds.
C. It is contraindicated in someone who is immunosuppressed.
D. Can be given to someone with an acute infection.
Answer and interpretation
A, pain, swelling and redness can occur in up to 10% but can rise to 50-80% if further tetanus toxoid is given. 60% of patients over the aged of 70 years actually have a poor immunity to tetanus. Those who are immunosuppressed may actually need a further dose due to their inability to create sufficient antibodies. Acute infection is a contraindication to all vaccines.
Q4. Which of the following is true for the tetanus vaccine?
A. Patients with burns are not at risk for tetanus.
B. Tetanus can be controlled via herd immunity.
C. Any reaction to a tetanus shot means further doses can not be given.
D. Severe reactions to tetanus vaccine usually indicate a high -pre-existing antitoxin level.
Answer and interpretation
D, patients with burns are at significant risk due to a break down of the bodies natural defence. Tetanus cannot be controlled via herd immunity due to its ubiquitous presence in the soil. The only contraindication to further tetanus toxoid is proven anaphylaxis. Severe reaction can occur if there are high levels of antitoxin present.
Q5. Tetanus facts:
A. Worldwide incidence is 1 million.
B. Benzylpenicillin is the mainstay of treatment once the patient has a confirmed diagnosis.
C. Incubation is rapid, less than 12 hours.
D. Tetanus spores last 1-2 weeks in the soil.
Answer and interpretation
A, In 2011 0.5 – 1 million cases occurred worldwide. Benzylpenicillin should not be used due to its GABA antagonism, metronidazole is the mainstay of antibiotic therapy. Incubation periods vary, it can be rapid within 24-48hrs with wounds on the face (cephalic tetanus) but as long as 21 days and even cases out to 3 months. Spores stay in the soil for years.
Q6. Tetanus facts:
A. Spasms are common initially but do not cause significant pain.
B. Risus sardonicus can be present.
C. Neonatal transmission is through wounds from C-sections.
D. Anti-tetanospasmin immunoglobulin is worthless once the disease is clinically present.
Answer and interpretation
B, Spasms are common but are often painful and can occur with minimal stimuli, e.g. a draft. Risus sardonicus is the name given for facial spasms, sometimes also seen with strychnine poisoning. Neonatal transmission is from infected umbilical stumps. It is practise in some countries to aid healing of the umbilicus and prevent bleeding by placing animal dung on the umbilical stump, 10 days later clinical signs of neonatal tetanus can be present. Anti-tetanospasmin Ig and post-exposure prophylaxis with tetanus toxoid should be given as soon as possible as well as metronidazole.
Q7. Tetanus facts:
A. Modern supportive care and treatments can lower the mortality from 60% to 2-3%.
B. Human tetanus Immunoglobulin dose is 105 IU intramuscularly.
C. It can always be identified by wound swabs.
D. The toxin inhibits NMDA receptors.
Answer and interpretation
A, this is true, including antibiotics, immunoglobulin, tetanus toxoid, +/- tracheostomy, assisted ventilation and muscle relaxants. The dose of human tetanus immunoglobulin is 150 IU/kg intramuscularly, the dose stated is for equine immunoglobulin. Tetanus bacteria are recovered from wounds in less than 30% of cases, also blood and CSF are usually normal during attacks. The toxin inhibits GABAergic and glycine mediated motor-neurones.
References
- Beeching N and Gill G. Lecture Notes – Tropical Medicine. 7e Wiley Blackwell 2014.
- Eddleston, Davidson, Brent, Wilkinson. Oxford Handbook of Tropical Medicine. Oxford Medical Handbooks. 4e 2014
- Matthews PC. Tropical Medicine Notebook. Oxford University Press, 2017
- The green book – tetanus
- WHO immunisation poster
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.