
![]()
The Dirty Dozen
The Dirty Dozen: Common Errors On Discharging Patients Recovering From Critical Illness
This post is co-authored by the following team of clinicians and researchers:
- Theodore J Iwashyna, MD, PhD (VA Ann Arbor and University of Michigan); Twitter: @iwashyna
- Andrea B Johnson, APRN (Mayo Clinic); Twitter: @abj2280
- Joanne McPeake (Glasgow Royal Infirmary); Twitter: @Jomcpeake22
- Jakob McSparron (University of Michigan); Twitter: @Jakob_McSparron
- Hallie C Prescott, MD (VA Ann Arbor and University of Michigan); Twitter: @HalliePrescott
- Carla Sevin (Vanderbilt University); Twitter: @ICU_Recovery
- Chelsea Harris – #CoVisual; (University of Maryland);Twitter @CAHarrisMD
DISCLAIMER: “These do not necessarily represent the views of the U.S. Government or Department of Veteran Affairs.”
Introduction
Over a decade working with patients recovering from acute respiratory failure, sepsis, and acute respiratory distress syndrome (ARDS), it has become clear that there are common, avoidable, recurring errors in their care. With COVID-19, lots of clinicians are surging into unfamiliar roles, with a very high operational tempo. This is a perfect set-up for an outbreak of these common mistakes.
To help clinicians who are preparing recently mechanically ventilated patients for discharge, we offer this Dirty Dozen questions to ask. They arise not from judgmentalness, but from the reality that we have all made these mistakes, and we hope by discussing them frankly, it will be easier for you not to repeat our errors. Certainly there are other possibilities to which astute clinicians attend, but here are a high-yield dozen to start with.
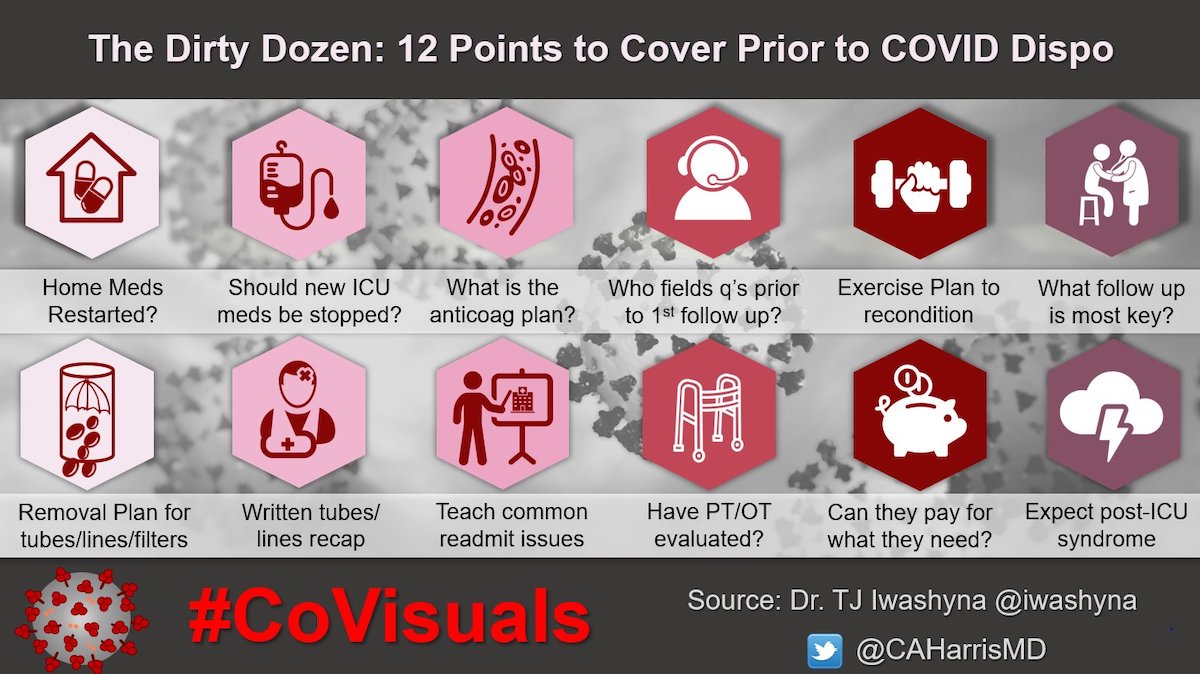
The Dirty Dozen
1. Are their home medications (mostly) restarted? It is very common for medications like antihypertensives, statins, inhalers, and Synthroid to get dropped in the ICU for transient reasons, and often they should be restarted.
- If their blood pressure, blood sugars, weight, or creatinine are not yet back to normal, have their meds been titrated? And who will continue to adjust the meds over the coming weeks as they continue to heal?
- For this and all other follow-up questions: Is that plan realistic given how hard it is to see a primary care provider right now?
2. Do they need to be on that anti-psychotic, PPI, H2 blocker, “sleep aid”, or opiates? Often these get started in the ICU for transient reasons, and unless there is a good individualized reason to keep them, they should be stopped.
3. What’s the plan for anticoagulation? There is a lot of empiric anticoagulation for COVID19 being used in the ICU. Was it empiric, or was a clot found? Who is going to own the monitoring and duration decisions in the outpatient setting, and how are the key inpatient data being handed off?
4. What is the plan for who the patient should call in the event of new issues that arise prior to their first primary care provider visit?
5. Have you encouraged patients to gently push themselves to move and exercise? Deconditioning and fatigue will be a real problem, but a little dyspnea or discomfort is a sign of exercise working—otherwise people risk simply sitting on the couch getting weaker. Moderation is good; immobility is bad.
6. Are the lines and “temporary devices” all out? Especially femoral lines and temporary IVC filters are at risk for getting left in.
7. Do they have a written list of all lines/tubes/drains that they had this hospitalization? They need to know what the different bumps and bruises and holes are from and what to look for regarding healing/infection risk.
8. What are the absolutely key follow-up they need? Follow-up is going to be really hard in the current environment, but please pick the 1-3 things they really must do, and make sure they are set-up BEFORE they leave the hospital. Ask: should that include specific nutritional support?
9. We know the top 5 reasons patients get readmitted after severe infections and sepsis. Have you educated your patient and their family about how to respond to early signs of (1) repeat infection, (2) congestive heart failure, (3) aspiration, (4) acute kidney injury, and (5) a COPD exacerbation?
10. Has occupational or physical therapy seen the patient? Combinations of weakness and confusion are very common after ICU. Patients + caregivers can learn adaptations from OT/PT
11. Can they pay for the follow-up they will need? With the rise in unemployment + often already stingy insurance, you can ask social work to insure they will really get the medications, physical therapy, basic food, and equipment they need to keep getting better at home.
12. Have you given them information about the Post-Intensive Care Syndrome? – see the handout from the American Thoracic Society at https://www.atsjournals.org/doi/pdf/10.1164/rccm.2018P15 Great online support is available at https://connect.mayoclinic.org/page/pics/tab/resource-77/ that can also help them find other peer support
References
- Bell, C. M., et al. (2011). Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA 306(8): 840-847.
- Brown, S. M., et al. (2019). Approaches to Addressing Post-Intensive Care Syndrome among Intensive Care Unit Survivors. A Narrative Review. Ann Am Thorac Soc 16(8): 947-956.
- Chopra, V., et al. (2014). Do clinicians know which of their patients have central venous catheters?: a multicenter observational study. Ann Intern Med 161(8): 562-567.
- Tammy L. Eaton, Joanne McPeake, Julie Rogan, Annie Johnson, Leanne M. Boehm; Caring for Survivors of Critical Illness: Current Practices and the Role of the Nurse in Intensive Care Unit Aftercare. Am J Crit Care 1 November 2019; 28 (6): 481–485. doi: https://doi.org/10.4037/ajcc2019885
- Haines KJ, Sevin CM, Hibbert E, et al. Key mechanisms by which post-ICU activities can improve in-ICU care: results of the international THRIVE collaboratives. Intensive Care Med. 2019;45(7):939–947. doi:10.1007/s00134-019-05647-5
- McPeake, J. M., et al. (2019). Social and economic problems of ICU survivors identified by a structured social welfare consultation. Crit Care 23(1): 153.
- McPeake, J. M., et al. (2019). Exploring Patients’ Goals Within the Intensive Care Unit Rehabilitation Setting. Am J Crit Care 28(5): 393-400
- Prescott, H. C., et al. (2015). Readmission diagnoses after hospitalization for severe sepsis and other acute medical conditions. JAMA 313(10): 1055-1057.
- Prescott, H. C. and D. C. Angus (2018). Enhancing Recovery From Sepsis: A Review. JAMA 319(1): 62-75.
- Scales, D. C., et al. (2015). Unintentional Continuation of Medications Intended for Acute Illness After Hospital Discharge: A Population-Based Cohort Study. J Gen Intern Med
- Sevin, C. M., et al. (2018). Comprehensive care of ICU survivors: Development and implementation of an ICU recovery center. J Crit Care 46: 141-148
- Stollings, J. L., et al. (2018). Critical Care Pharmacists and Medication Management in an ICU Recovery Center. Ann Pharmacother 52(8): 713-723.
[cite]

Critical Care
Compendium

Critical care physician and health services researcher bringing the tools of social science and outcomes research to improve the care of patients with critical illnesses. I practice as an intensivist at the University of Michigan’s and the Ann Arbor VA's Critical Care Medicine units, where we work to bring the latest science and the best of clinical practice to patients | iwashyna-lab | @iwashyna |