
![]()
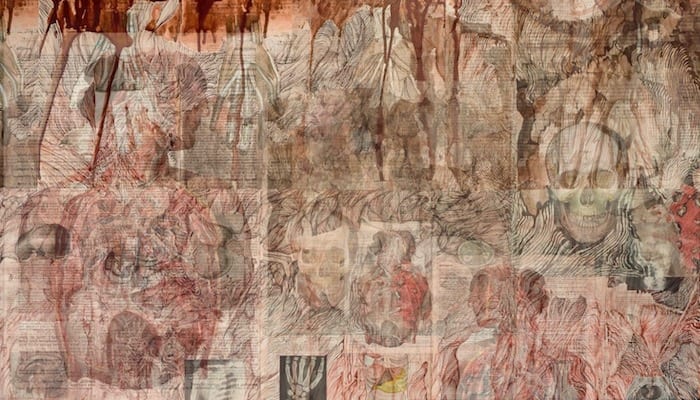
The Half Moon Nail
aka Bone and Joint Bamboozler 006
40 year old male attends with acutely painful toe following a weekend DIY incident.
[Sledgehammer 1 – Man 0]

What is the diagnosis?
Bamboozler Answer
Subungual Haematoma
- Subungual haematomas occur when there is bleeding beneath the nail. Generally caused traumatically by getting it caught between to hard surfaces.
- The haematoma becomes trapped between the rigid structures of the nail above and the distal phalanx below.
- The space occupying mass causes intense pain secondary to increased pressure against the very sensitive nail bed and matrix.
How would you assess this injury?
Bamboozler Answer
Examination should include:
- Testing extensor and flexor tendons
- Testing circulation by capillary refill
- Checking the sensitivity to the area
Investigation:
- X-rays are generally indicated to rule out crush injury or fracture to the distal phalanx
- Document the percentage of nail bed covered by the haematoma, surrounding damage to tissues, nail-bed, and nail margins.
What are the potential complications?
Bamboozler Answer
- Fracture to the distal phalanx
- Crush injury
- Nail bed injury
- Performing trephination on subungual ecchymosis.
If no history of trauma or story doesn’t fit with subungual haematoma consider melanoma, Kaposi’s sarcoma, and other tumors.
What are the treatment options?
Bamboozler Answer
Wait and See:
Patients who are not experiencing significant pain at rest, should not have trephination performed, and can be treated with simple analgesia, rest, ice, and a protective splint.
Trephination:
Trephination gives good cosmetic and functional result in both adults and children as long as no other fingertip injury is present.
Trephination makes a closed wound open, and introduces the risk of bacteria entering causing infection, once procedure completed and haematoma evacuated no need to further soak digit, and a protective dressing should be applied for 7-10 to prevent infection.
LITFL: Subungual haematoma trephination. Procedure
References
- Bonistereel, P. (2008). Trephining subungual hematomas. Canadian Family physician. 54, 693.
- Cadogan M. Subungual haematoma trephination. LITFL
- Sherman, S. Simon’s Emergency Orthopedics 7e
- Purcell, D. Minor Injuries A Clinical Guide 3e
CLINICAL CASES
Bone and Joint Bamboozler
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
Hi Chris,
is the any time frame to do trephination ?
Hi
According to Roberts and Hedges: “The blood usually remains fluid for 24 to 36 hours and is easily expressed with slight pressure.”
Cheers
Chris