
![]()
The Paradoxical Alternative
aka Cardiovascular Curveball 006
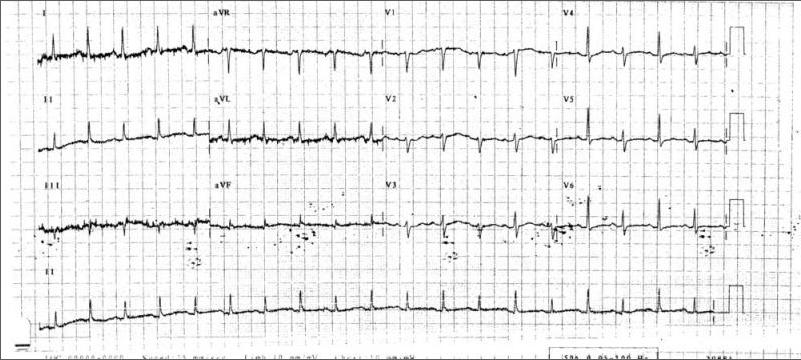
Consider a 49 year-old female with a history of smoking and two weeks of increasing shortness of breath. She is being treated for pneumonia on the ward for three days but getting worse. An ICU review is performed on the ward and the following ECG is obtained.
Q1. Describe the ECG findings. What investigation is indicated?
Curveball Answer
The most significant finding on this ECG is the presence of electrical alternans.
The rhythm is sinus tachycardia at 100/min and the axis is normal.
The investigation indicated is an echocardiogram to confirm the presence of a pericardial effusion and to look for echocardiographic evidence of pericardial tamponade.
Q2. You ring the cardiologist they ask you to assess the degree of pulsus paradoxus. What is pulsus paradoxus and what are the potential causes of this phenomenon?
Curveball Answer
Pulsus paradoxus is defined as an inspiratory drop in blood pressure of 10mmHgor more during normal breathing.
Pulsus paradoxus is caused by:
- pericardial tamponade
- hypovolaemia (especially during positive pressure ventilation)
- acute asthma
- massive pulmonary embolism
On the cardiologist’s advice you assess the degree of pulsus paradoxus and no significant respiratory variation in systolic pressure is present.
Check that the R-R interval on the ECG is regular to rule out arrhythmia as the cause of a fluctuating systolic blood pressure.
Q3. The cardiologist argues that the absence of pulsus paradoxus is reassuring. Are they right?
Curveball Answer
In this particular case, no.
Electrical alternans is usually associated with tamponade and there are many reasons why pulsus paradoxus may be absent in the presence of cardiac tamponade including:
- Pericardial adhesions (particularly over the right heart)
- impede volume changes
- Severe left ventricular failure or marked left ventricular hypertrophy
- in these circumstances the pericardial pressure effectively equilibrates only with the right heart pressures with the much less compliant left ventricle resisting phasically changing pericardial pressure
- Right ventricular hypertrophy without pulmonary hypertension
- causes right-sided resistance to the effects of breathing
- Atrial septal defects
- increased venous return balanced by shunting to the left atrium
- Severe aortic regurgitation
- produces sufficient regurgitant flow to damp down respiratory fluctuations
References
- Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003 Aug 14;349(7):684-90. PMID: 12917306.
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF

CLINICAL CASES
Cardiovascular Curveball
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC