
![]()
Think it’s just the flu? Think again
You learn early in medicine that you will never diagnose a disease that you don’t consider. We all suffer from tunnel vision, and this can result in misdiagnosis and ultimately significant morbidity for patients. Currently most of us are aware of the importance of a good travel history because of the recent Ebola virus outbreak that put everyone on heightened awareness for at least one continent hopping virus.
This is important because clinicians often assume that the acute onset of fever, sore throat, myalgias, headaches, and cough all point towards a diagnosis of influenza or an influenza-like illness (ILI). In many places in the United States, this would result in a prescription for Tamiflu and a discharge home regardless of the results of a flu swab, as it was in the case reported in this article. I’ll not discuss the evidence behind oseltamivir, but the fact of the matter is that patients want it and physicians give it. Nonetheless, the majority of the time the clinician would probably be right (or at least not horribly wrong).
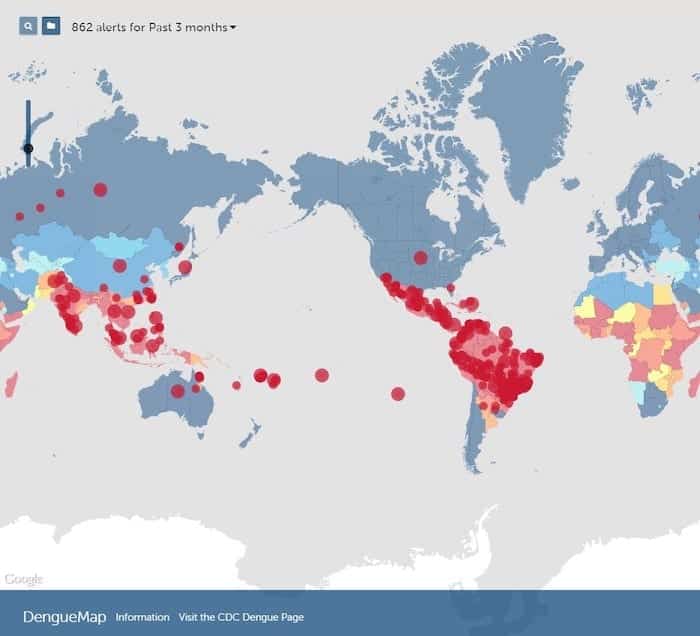
This is all well and good, except that this patient didn’t have influenza. She actually had dengue, which she had picked up on a trip to Haiti that ended 7 days prior to presentation, consistent with the normal incubation period of 3-14 days.
Why does this matter? Because while dengue fever may not be necessarily life threatening, if it progresses to dengue hemorrhagic fever or dengue shock syndrome it certainly carries a worse prognosis. Typically this occurs in those previously infected, so a asking if there has been a prior diagnosis of dengue is also important. Then how do you distinguish between the two?
Clinically, one sign that can point in the right direction is that dengue can cause a truncal rash, which is uncommon in flu. Another vaguely nonspecific clinical finding is a bimodal or “saddleback” fever that persists for 3 days, resolves, and peaks again in 1-2 days. Typically most symptoms resolve in a week, barring severe complications.
Also, apart from dengue titers, most labs are nonspecific in distinguishing dengue from influenza. Both can cause elevations in CPK, transaminases, and the acute phase reactants (ESR and CRP). Both can also cause leukopenia and thrombocytopenia. One finding that is relatively specific is markedly elevated serum ferritin, which can also be elevated for Legionnaire’s disease, another ILI.
In the end, treatment of dengue is no different from that of influenza, mainly supportive care. People infected with dengue are more likely to result in hospital admission, so appropriate suspicion and testing may prevent the “bounceback” patient who ends up getting admitted. Proper diagnosis of dengue is also necessary for epidemiologic purposes. And while your febrile returning traveler might not have dengue either, you still need to make sure their ILI isn’t leptospirosis, MERS-CoV, Legionnaire’s, measles, malaria, meningococcal disease, or typhoid. Thus, keep an open mind, as those hoofbeats might be horses, zebras, or unicorns.
References
- Cunha BA, Raza M. During influenza season: all influenza-like illnesses are not due to influenza: dengue mimicking influenza. J Emerg Med. 2015 May;48(5):e117-20. [PMID 25736548]
- Dengue control. WHO

EBM Gone Wild
Wilderness Medicine
Emergency physician with interests in wilderness and prehospital medicine. Medical Director of the Texas State Aquarium, Padre Island National Seashore, Robstown EMS, and Code 3 ER | EBM gone Wild | @EBMGoneWild |