
![]()
Ultrasound Case 051
Presentation
A 61 year old woman is reluctantly brought into your Emergency Department by an anxious relative with weight loss and lethargy. She has noticed a mass in her right upper quadrant that has been there for several months.
You put the ultrasound probe on over the palpable mass.
View 2 and 3
Describe and interpret these scans
IMAGE INTERPRETATION
Image 1: Longitudinal view of the gallbladder.
The GB is markedly and irregularly thickened and echogenic, but not striated and oedematous as one sees in cholecystitis. It is non tender. It contains several large calculi. There is a trace of pericholecystic fluid.
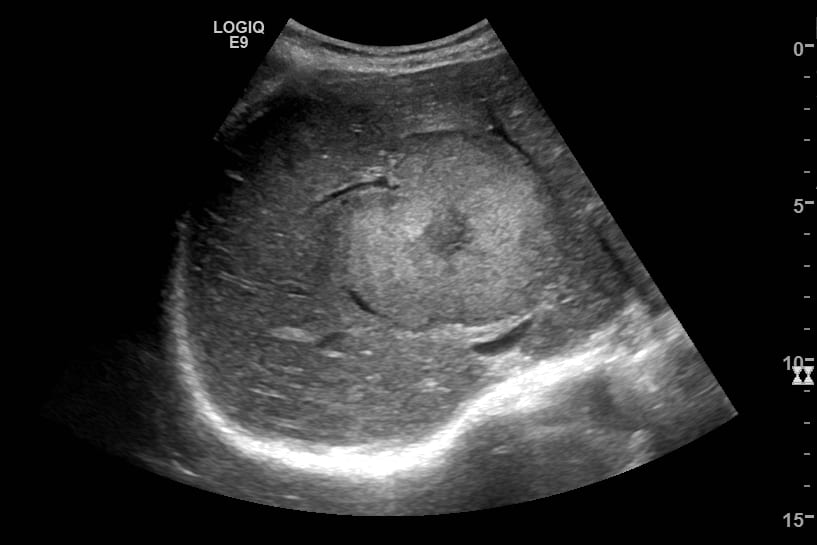
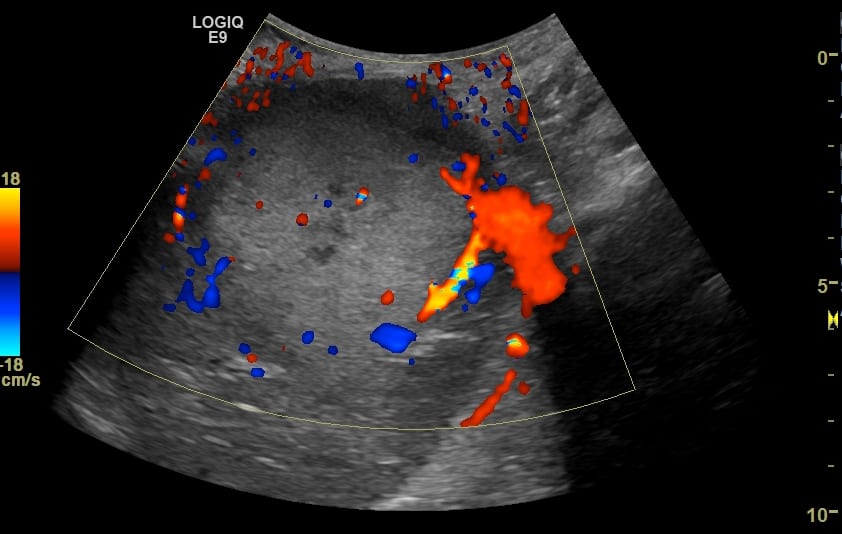
Image 2 & 3: Transverse view of the right lobe of the liver (with Doppler).
A large rounded lesion measuring about 6cm across is seen centrally. It distorts the underlying hepatic architecture and vascualture. It has a targetoid appearance. There is a thin hypoechoic halo, then the bulk of the lesion is echogenic and finally there is a central hypoechoic area likely to represent central necrosis.
The lesion demonstrates some peripheral vascularity but is not highly vascular. It is almost certainly a metastasis from the gallbladder lesion.
CLINICAL CORRELATION
Malignancy of the gallbladder with liver metastases.
Differentiating the causes of gallbladder wall thickening can be difficult and clinical correlation is essential.
Here is a thickened gallbladder wall with gallstones and pericholecystic fluid but it is not cholecystitis.
A very thickened gallbladder wall from acute inflammation tends to be oedematous and striated and there is usually debris either suspended or dependent within the GB lumen. Here the very solid appearance with anechoic bile and a non tender GB, as well as the liver metastases and accompanying clinical history make the diagnosis of gallbladder malignancy with liver secondaries most probable.
Cancer involving the gallbladder may be itself be primary or metastatic. When primary, involvement may be focal or diffuse.
Histologically primary gallbladder cancer is usually adenocarcinoma (90%) or less commonly squamous carcinoma. This case was a small cell neuroendocrine tumour which only makes up about 2% of gallbladder cancers but is well described in case series in the literature. It is most frequent in older women and has poor prognosis, with spread beyond the GB common at presentation.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |