
![]()
Ultrasound Case 087
Presentation
A 28 year old with reduced GCS after several seizures requires intubation. Their neck extension seems limited and you wonder whether this may be a difficult intubation. You decide to monitor it with ultrasound.
Describe and interpret these scans
IMAGE INTERPRETATION
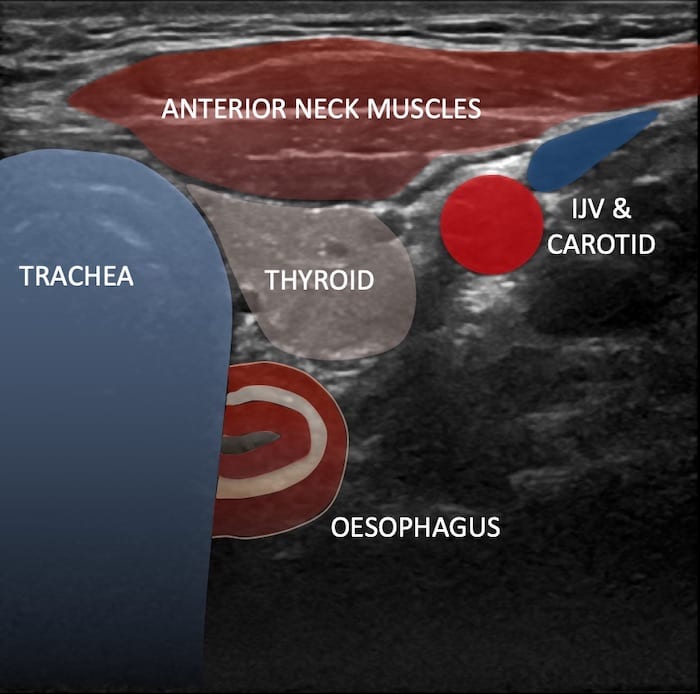
Image 1: Transverse view of lower neck centre and left.
The Trachea is seen, with the characteristic bowel wall signature – the oesophagus is peeking out from behind the left as it usually does. You wait and watch as the intubation proceeds. You wait for a flutter as the deflated cuff moves through the cricoid cartilage and into the tracheal rings. But on this occasion there is sudden movement and appearance of the tube in the oesophagus. It looks like there are two tracheas. The ultrasound operator quickly notifies the operator (prior to bagging) who removes the tube are carefully replaces into the trachea, this time with the guidance of a video laryngoscope and a bougie.
View 2: Tracheal intubation
CLINICAL CORRELATION
Oesophageal intubation
There are several ways of ensuring endotracheal intubation but in competent hands ultrasound visualisation has several advantages.
- Feedback is given in real time so there is no need to ventilate or to wait for end tidal CO2.
- The operator can press gently with the probe creating cricoid pressure if desired or can use it to guide the larynx – if laryngeal manipulation (like “BURP”) if required.
- It is easy to visualise oesophageal intubation whilst it is more difficult to see tracheal intubation – however success can be inferred if the tube is passed and the oesophagus not intubated.
- Lung sliding can also be used to confirm ventilation of both lungs once the tube has passed.
I use the linear transducer. It can also be used to rapidly locate and mark the cricothyroid membrane if required – although this should be preempted and done before a failed attempt at intubation rather than once a “can’t oxygenate, can’t ventilate” situation has been reached.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |